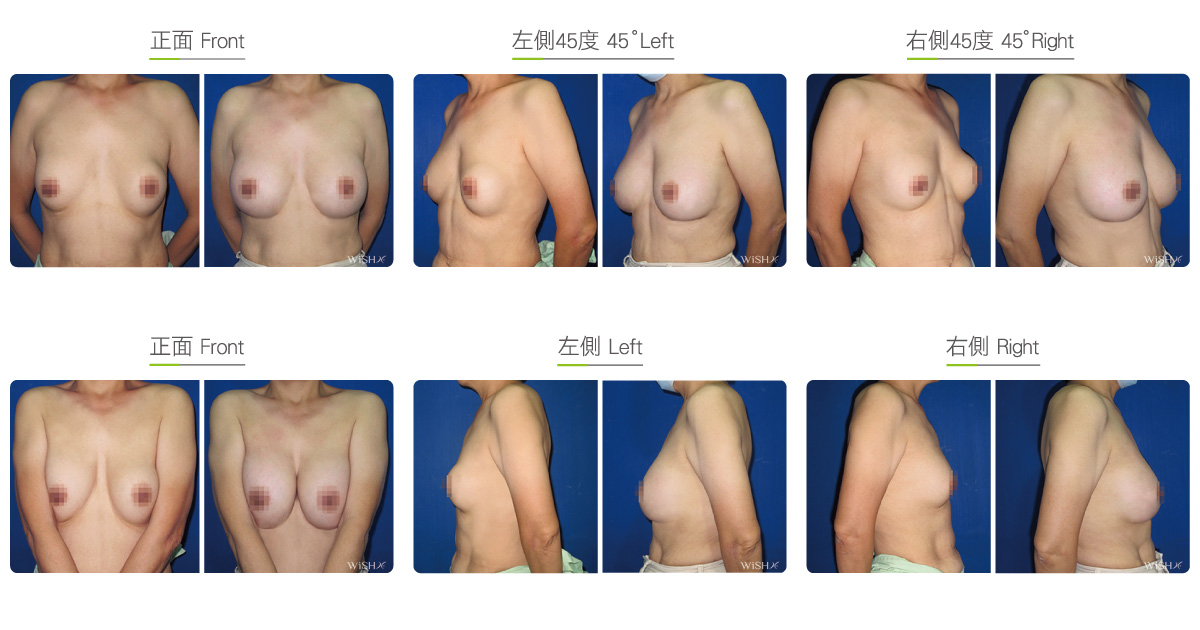
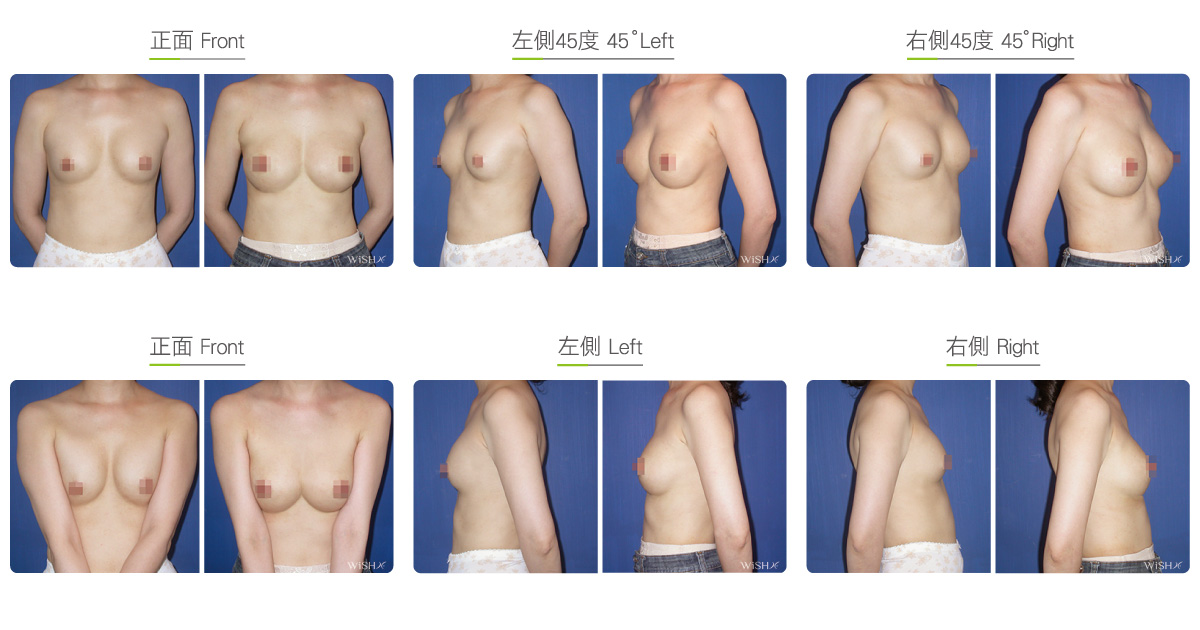
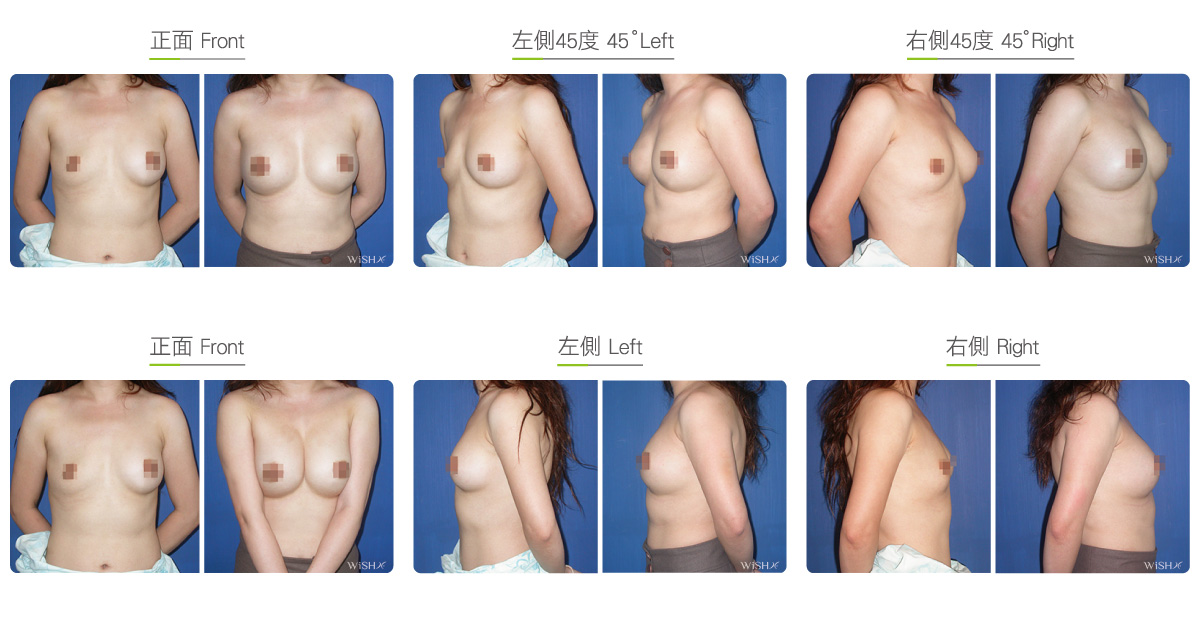
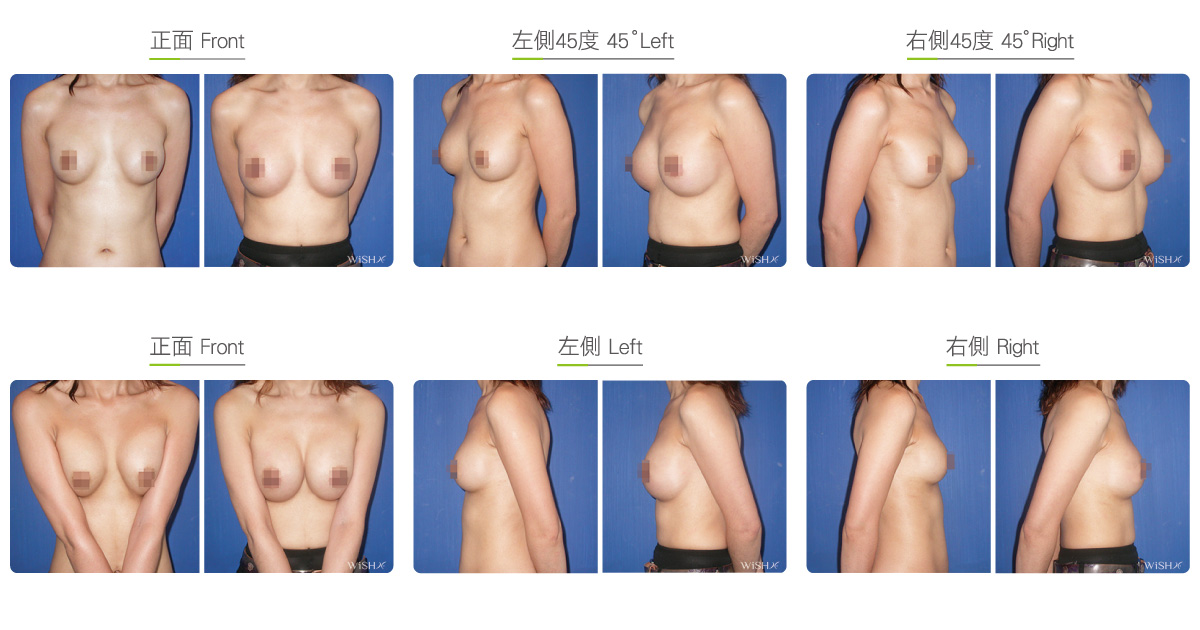
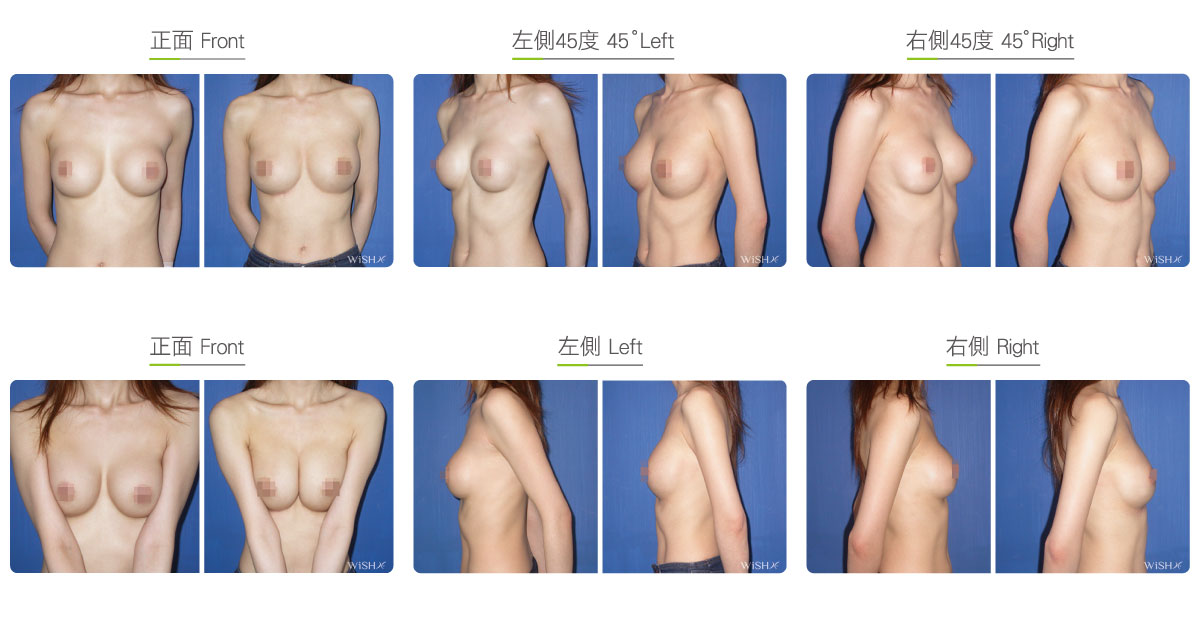
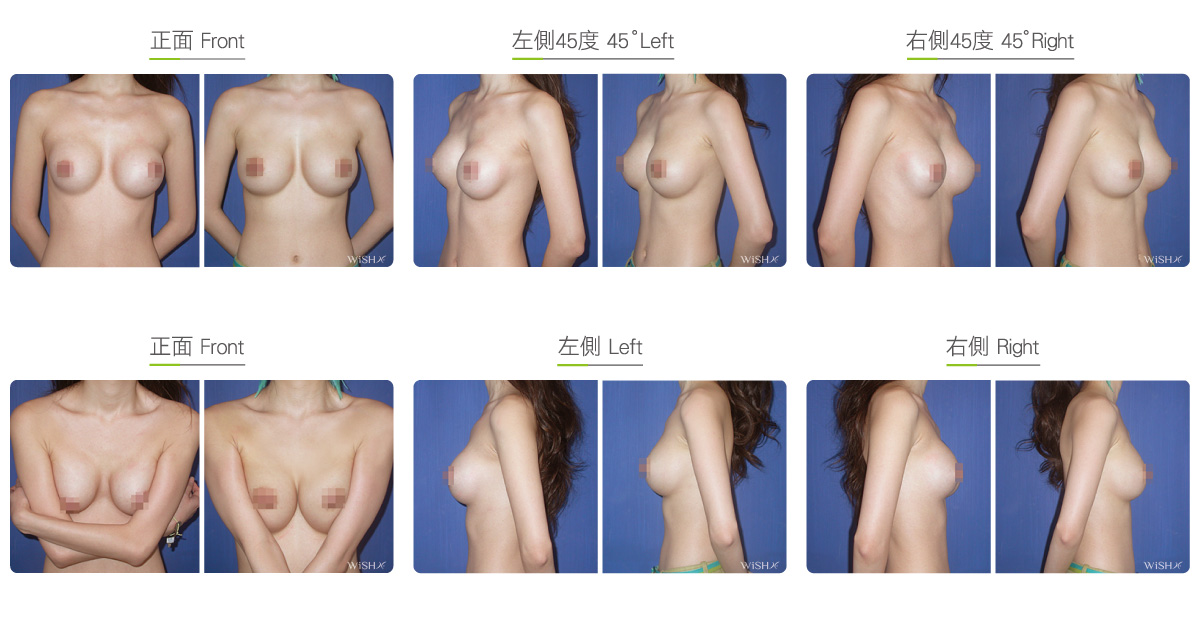
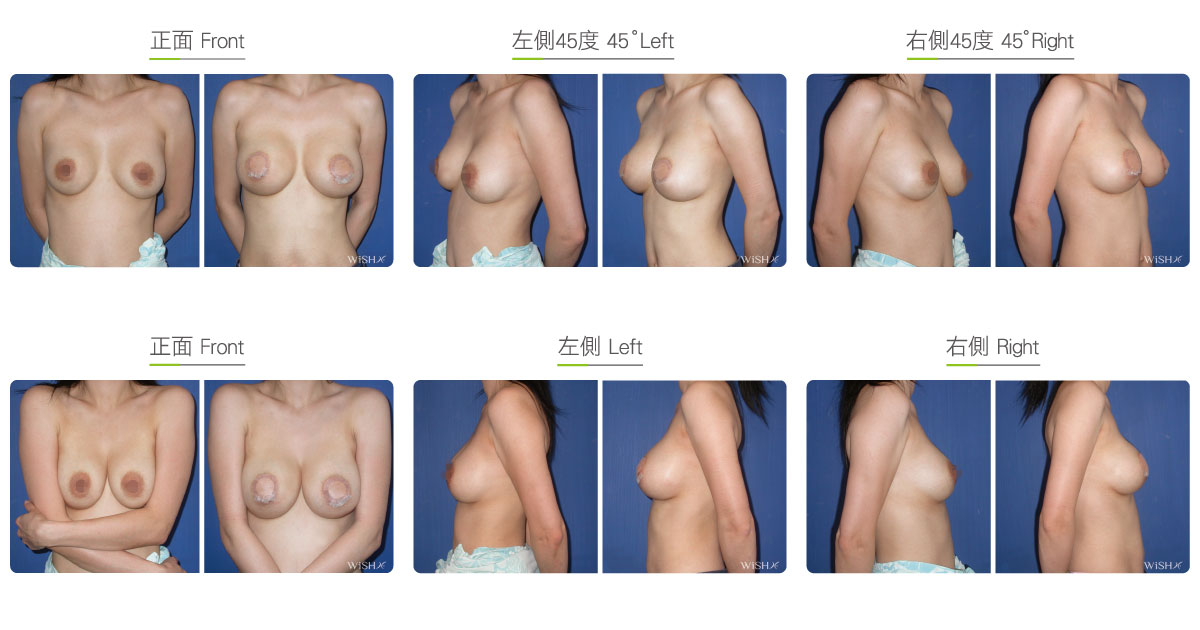
Capsulectomy
This is the most effective solution for severe (grade 4) capsular contracture. It completely removes contracted, thickened capsules with implants, restoring a pocket back to its soft and spacious state of first surgery, and then places new implants. The surgery can be performed with a transaxillary, a periareolar, or an inframammary incision. First, endoscopy and ESUs are used to completely separate capsules from normal breast tissue. The whole capsule is removed with original implants, and ESUs are used to remove the remaining fibrotic scar tissue and dissect a new pocket space. Finally, new implants are placed to complete the surgery. This surgery is advantageous in that recurring or refractory capsular tissue can be completely avoided and that skin elasticity is restored. Without the influence of the remaining capsule or scar, the success rate of this method increases. However, this surgery is long and complex with more intraoperative and postoperative bleeding and a longer recovery period, adding more uncertainty to postoperative care. Patients’ skin may become loose and thin due to capsulectomy. Thus, for patients with less than ideal conditions or for those with repeated operations, problems such as breast ptosis or implant marginal puckering may be observed, which frequently entails replacement with larger implants to support breast tissues.
Surgical conditions
Duration
- Type of anesthesia: General anesthesia
- Type of incision: Previous incision or transaxillary, periareolar, or inframammary incision
- Recovery: Within 5–7 days
- Removal of stitches: 10–14 days
General instructions
No food and water on the day of surgery
- Temporary indwelling of a drainage tube is required to drain blood and liquid.
- Tasks and exercises that require excessive arm strength should be avoided for 1 month postoperatively.
- Smoking and consumption of collagen or vitamin C should be avoided for 3 months postoperatively to prevent the formation of capsules.
- Underwired or push-up bras should not be worn for 3 months postoperatively.
- Breast massage should be performed for at least 6 months postoperatively.
Ideal candidates
- Those with severe capsular contracture (grade 3-4)
- Those with evidently deformed or hardened (stone-like) breasts.
- Those with hardened breasts due to bleeding or infection from previous surgery.
- Those concerned about potential implant infection.
- Those concerned about the recurrence of capsular contracture.
- Those with repeated surgeries or refractory contracture.
Possible complications
- Hematoma
- Infection
- Seroma
- Scar adhesion
- Implant leakage or rupture
- Uneven breast height
- Capsular contracture recurrence
- Hyposensitive nipples
- Implant leakage or rupture
Surgical advantages
-
Immediate results
-
Removal of capsules effectively reduces the chance of recurrence.
-
Eliminates concerns of capsule infection.
-
Increases pocket space and restores skin elasticity.
-
Easier and more stable postoperative care.
-
New implant size and placement method may be selected.
Surgical drawbacks
-
More invasive and complex surgery; slower recovery
-
Longer surgery; access by original incision is prone to incur scar adhesion
-
More prone to bleeding or swelling; indwelling of a drainage tube to discharge blood and liquid
-
Possibly thinner or looser skin after surgery
-
Larger implants needed to support the breast tissue after capsule removal
Possible procedures in conjunction
Comparison between Capsulotomy and Capsulectomy
| Capsulotomy | Capsulectomy | |
|---|---|---|
| Ideal candidates | Patients with mild to moderate (grade 2-3) contracture, unilateral hardening, or asymmetry | Patients with moderate to severe (grade 3-4) contracture, severe breast deformation or hardening, or recurrent contracture |
| Method of operation | Incision of capsules; original implants can be retained | Complete excision of capsules with implants; new implants needed |
| Type of operation | Revision at the original plane | Revision at the original plane |
| Range of operation | Mostly unilateral | Unilateral or bilateral |
| Duration of surgery | 1–1.5 h (one side) | 3.5–4 h (both sides) |
| Anesthesia | IV sedation or general anesthesia | General anesthesia |
| Size of implant | Original size can be kept | larger implants are necessary |
| Intraoperative bleeding | Less | More in most cases |
| Postoperative pain | Low | Slightly high |
| Postoperative blood draining | Might not be required | Necessary |
| Recovery | Fast | Slow |
| Loosening of skin | Mild | More obvious |
| Recurrent capsules | Possible | Low possibility |
| Postoperative massage | Required | Required |