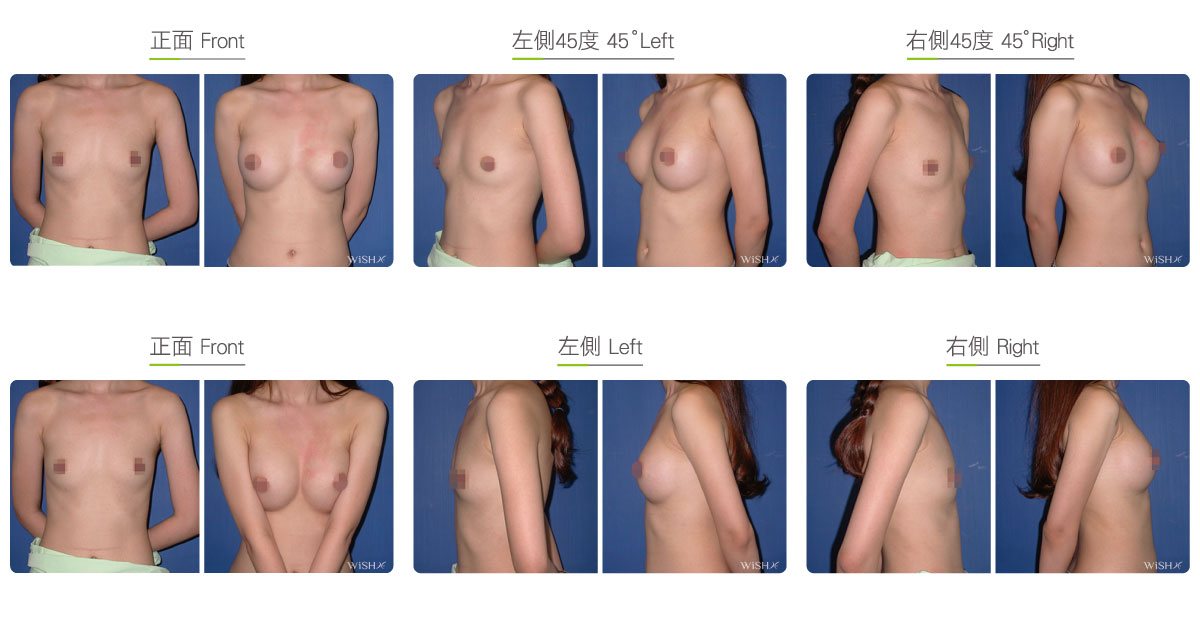
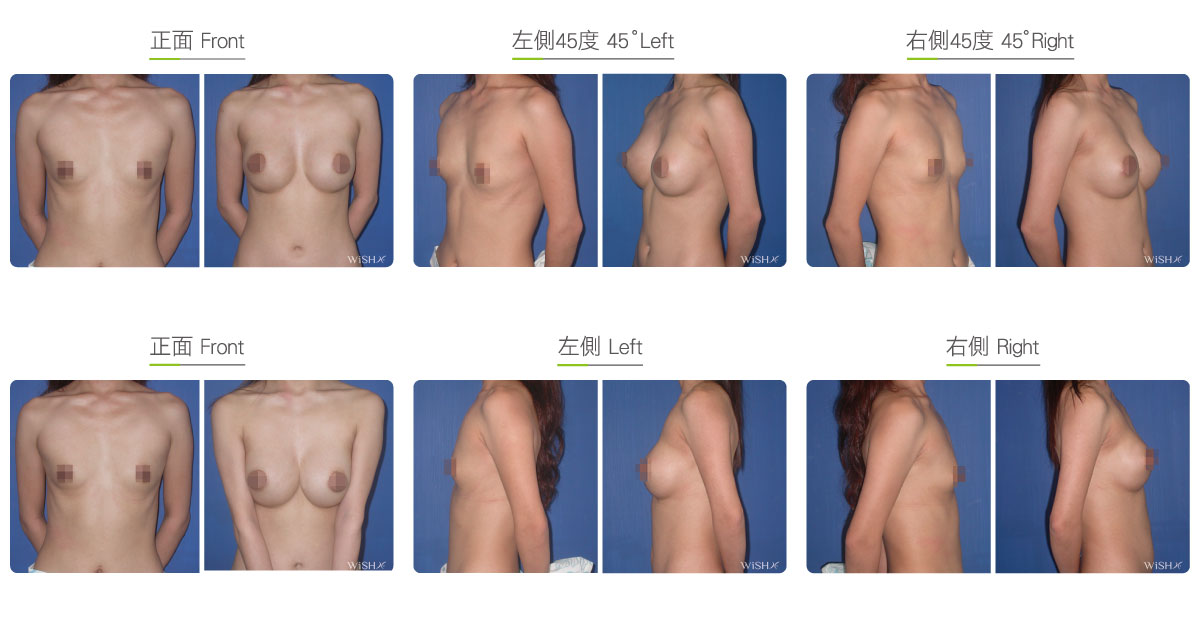
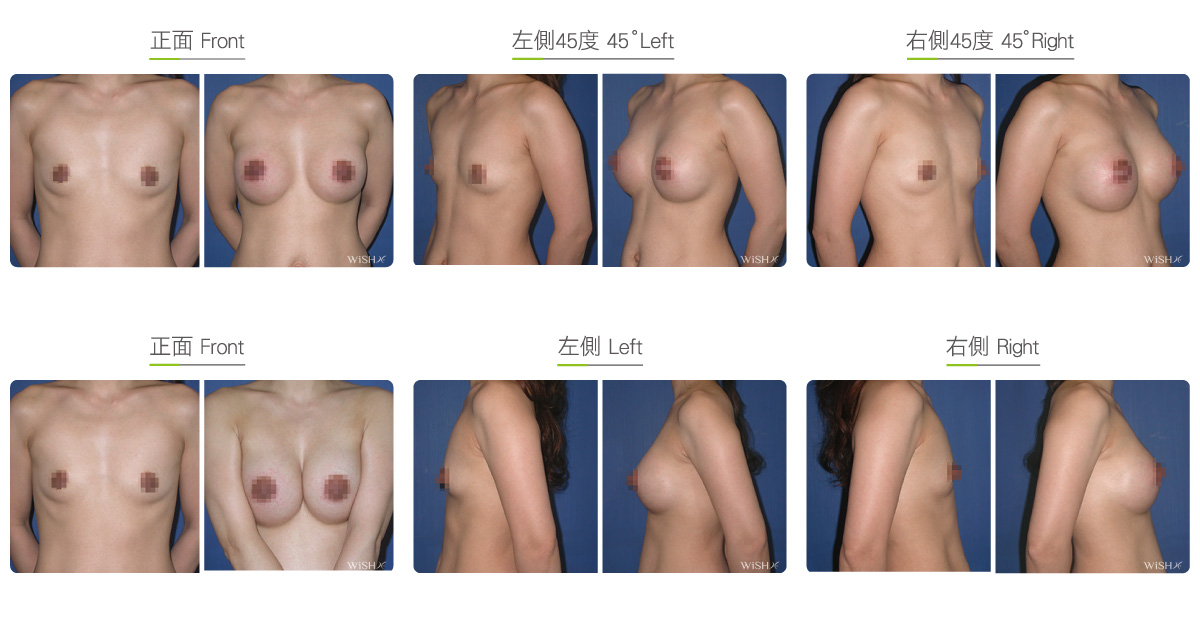
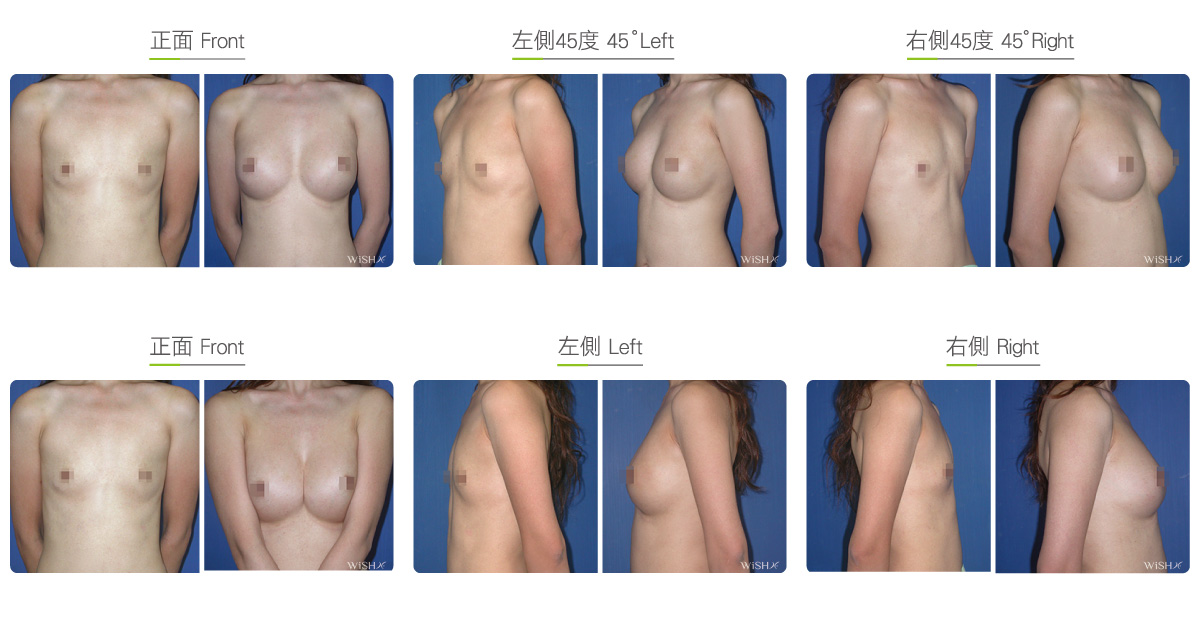
Subfascial Breast Augmentation
Subfascial placement is a new type of procedure whose popularity has increased in recent years with the widespread use of endoscopy. Implants are placed in the subfascial layer under the mammary gland tissue but on top of the pectoralis major muscle. The fascia is very thin in this area, only approximately 1–2 mm. Complete dissection in this plane would be very difficult to achieve without the aid of endoscopy; thus, the precision and complexity of this procedure are much higher than those of subpectoral surgery. It is a more advanced method of breast augmentation. The advantages of subfascial placement are that no crucial blood vessels or nerves are involved and that there is less damage to the muscle or tissue compared with that in the case of subpectoral placement. Thus, the recovery period is shorter, and there is much lesser pain after surgery. It is a modern and user-friendly breast augmentation procedure complying with human physiological characteristics and is ideal for patients afraid of pain.
Transaxillary, periareolar, or inframammary incisions can be used for subfascial placement. Implants are placed in the subfascial layer under the mammary gland tissue and on top of the pectoralis major muscle, a position that is closer to real breast tissue. This method not only allows the faster setting of shape but also can more easily create a natural teardrop shape or draping. In addition, the procedure does not require any cutting or damaging of muscle tissues and thus results in very little pain after the procedure or during massage. The postoperative care period can be shortened to 3–6 months. This surgery prevents implants from being affected by muscle contraction. Therefore, there are no restrictions on lifting weights or exercising with arms after surgery. On average, normal bras can be worn in 3 months, and no unusual movement of the breast due to muscle contraction is observed. However, this procedure is limited by conditions of the breast and skin. Patients must have thick enough breast tissue to cover implants to achieve a natural look and touch; otherwise, implant edges or ripples can be noticeable by touch because of the shallow placement. In addition, implant size should be moderated to avoid extra burden on the skin, which could result in premature breast sagging or unnaturally round breasts.
Surgical conditions
Duration
- Type of anesthesia: General or epidural anesthesia
- Type of incision: Transaxillary, periareolar, or inframammary incision
- Recovery: Within 2–3 days
- Removal of stitches: 7–10 days
General instructions
Fasting with no food and water before the procedure
- Frequent stretching should be performed for 1 month postoperatively to prevent axillary scar adhesion.
- Tasks and exercises that require excessive arm strength should be avoided, and underwired or push-up bras should not be worn for 1 month postoperatively.
- Smoking and consumption of collagen or vitamin C should be avoided for 3 months postoperatively to prevent the formation of capsules.
- Consistent and regular breast massage should be performed for 6 months postoperatively to maintain breast shape and softness.
Ideal candidates
- Those with original breast size larger than B cup
- Those with breast tissue thicker than 2 cm
- Those with chest skin thicker than 1 cm
- Those who have extreme fear of pain from surgery or breast massage
- Those who would like to reduce breast massage and care period
Possible complications
- Capsular contracture (<10%)
- uneven breast height
- scar adhesion (underarms)
- hypertrophic scarring (areola)
- implant leakage or rupture
- insensitive or oversensitive nipples (temporary)
Surgical advantages
-
Painless surgery and quick recovery
-
Easier postoperative massage with minimal pain
-
Care period can be shortened to 3–6 months
-
Faster and more natural setting of shape
-
No special restrictions on arm movement or lifting weights
Surgical drawbacks
-
Not ideal for those with thin body or skin.
-
Those with insufficient skin thickness could notice problems with touch such as feeling implant edges or ripples.
-
Too large implants could result in ball-shaped or unnatural breast shapes.
-
The procedure is compatible only with silicone implants (saline implants are more likely to have ripples).
-
Use of textured implants could be limited depending on patients’ conditions.
Possible procedures in conjunction
Comparison between Subfascial and Subpectoral Placement
| Subpectoral Placement | Subfascial Placement | |
|---|---|---|
| Ideal candidates | Those with naturally thin skin or a flat chest (A cup) | Those with thick skin tissue or a larger breast size (B cup) |
| Method of operation Implant placement |
Endoscopy is used throughout the procedure Under the muscle |
Endoscopy is used throughout the procedure Above the muscle |
| Choice of implant | Either saline or silicone | Silicone is preferred |
| Touch of implants | Less noticeable | More noticeable |
| Postoperative pain | Approximately 2–3 days | Not noticeable |
| Pain from massage | Approximately 1–2 weeks | Not noticeable |
| Duration of massage | Approximately ≥6 months | Approximately 3–6 months |
| Restriction on lifting weights | 3 months | 1 month |
| Wearing of normal bra | After 3–6 months | After 3 months |
| Incidence of capsular contracture | Higher (approximately 15%–20%) | Low (less than 10%) |
| Breastfeeding | Possible | Possible |