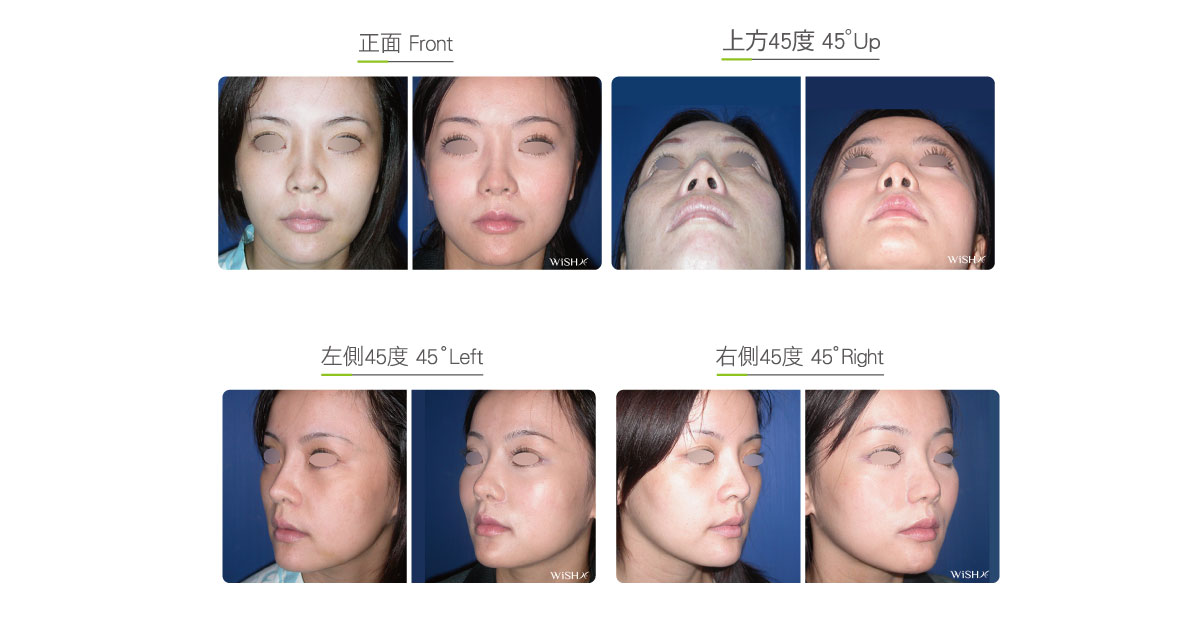
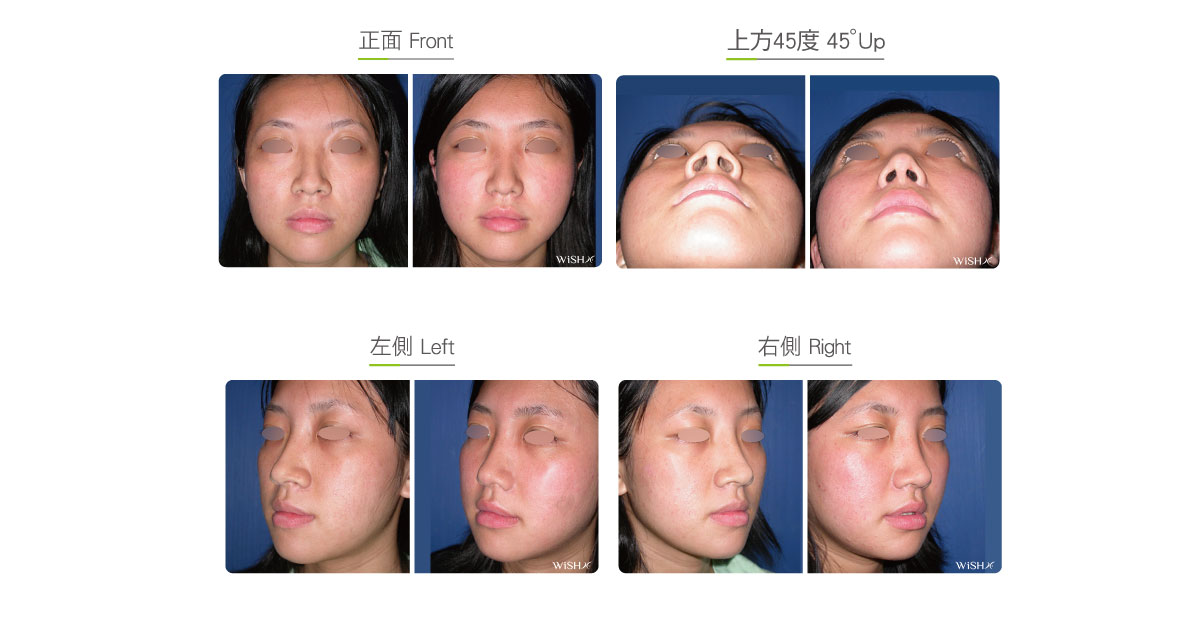
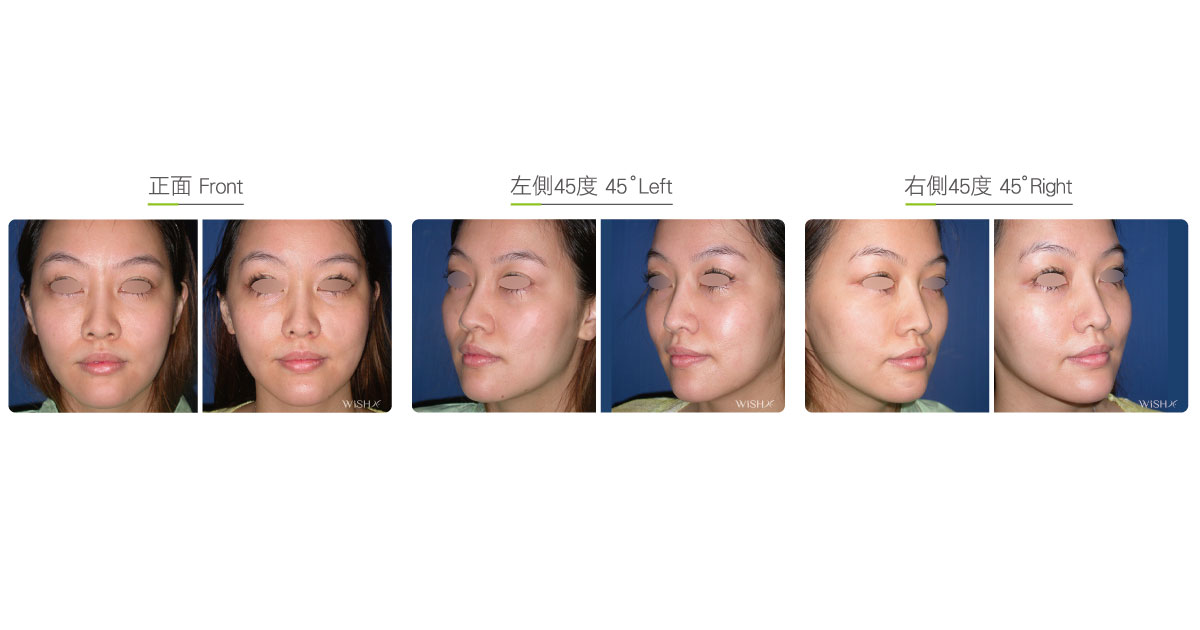
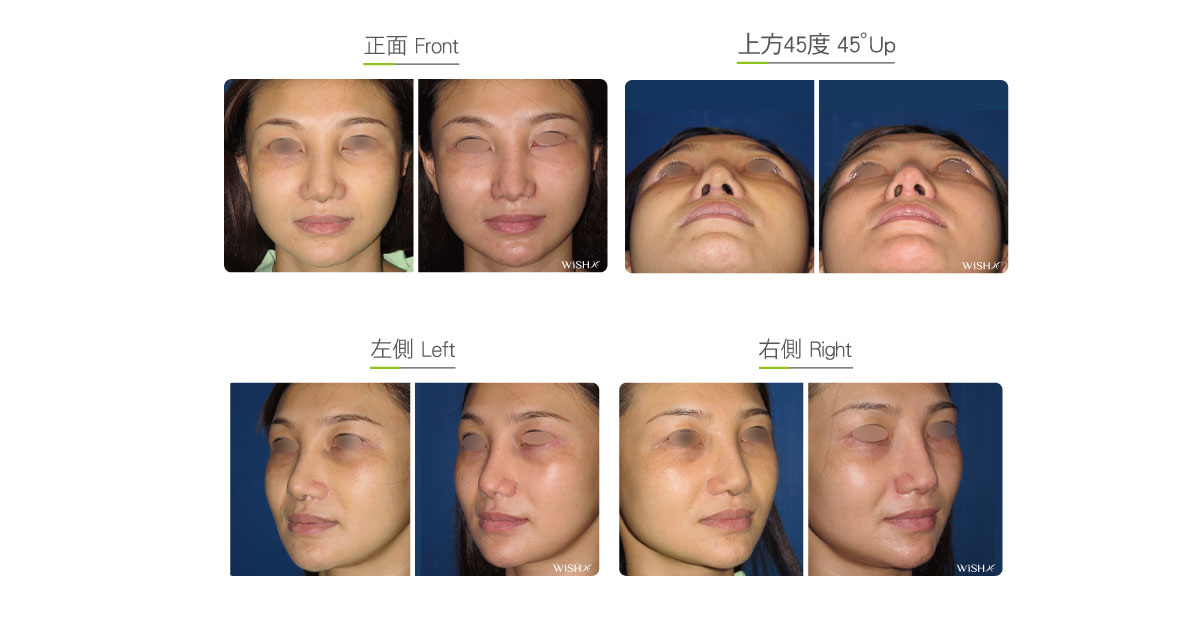
Alar Reduction
This is also called nostril reduction or alarplasty. The alar width is associated with the frontal visual area of the nasal tip, while its shape determines the nostril contour, so it plays a vital role in the overall evaluation of rhinoplasty. In accordance with the golden ratio of the face, the widest distance of the bilateral ala nasi should not exceed the span between the bilateral medial canthi (inner corner); otherwise, the patient will consider alar reduction. The other objective of alarplasty is to improve the shape and size of the nostrils by changing the nostril from an original circular shape to an oval shape and the alar feet direction from the preoperative toe-out to the postoperative toe-in shape, which prevents the widening of the ala nasi while speaking or laughing. Currently, the following two methods are available for ordinary alar reductions:
- Inner rim resection (scarless)
This is also called intra-alar sewing method or non-scar alarplasty. Surgery will excise the partial alar skin from the medial side of the ala nasi (inside nostrils) and then fixate the bilateral alar feet to the middle by passing a special suture through the bottom of the nasal columella, which narrows the bilateral ala nasi and simultaneously reduces the nostrils. The advantages of this surgery are to hide the scar, which is unnoticeable, inside the nostrils and the short surgical time and rapid recovery. Nevertheless, this method only alters the running of the ala nasi and does not reduce the nostrils much, so it is indicated for patients with an obvious toe-out ala nasi but not for those with an exceedingly wide ala nasi or big nostrils. Its shortcomings comprise the premature sloughing of internal stitches, resulting in the secondary dilation of the ala nasi. Besides, if the suture is too tight, the nostrils appear upturned or exposed and the facial expression would also be limited to make laughing impossible, therefore undermining the esthetics and naturalness of the surgery. - Alar base resection
This is an effective alar reduction and is indicated for a majority of patients with round and big nostrils or an exceedingly wide ala nasi. It is conducted by resecting the excess or exceedingly long alar skin via the inner margin of the nostrils till the outer margin of the alar feet. This surgery dramatically reduces the ala nasi and nostrils and also makes an adjustment to the position for the stitching to change the shape and height of the ala nasi, thus delivering relatively customized changes. Clinically, it is frequently integrated with open (Korean-style) rhinoplasty or open tiplasty to reinforce the overall satisfaction. Nevertheless, this method leaves a scar at the suture of the alar base and in patients with large pores or hypersecretion (seborrhea), which is relatively difficult to heal; therefore, attention should be paid to the scar care.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: Inside the nostrils (inner rim resection) or extended outward to the alar foot margin (alar base resection)
- Recovery: 1–2 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Try to avoid activities such as laughing and singing that may stretch the ala nasi for 1 month postoperatively.
- Avoid smoking and alcohol for 3 months postoperatively, and clean the intranasal wound every day in the morning and evening.
Ideal candidates
- Patients with a hypertrophic and wide ala nasi
- Those with obviously exposed or round and big nostrils
- Those with an unesthetic alar shape
- Those undergoing rhinoplasty due to a bulbous or plump nose
Potential complications
- Scar hypertrophy
- Excess reduction
- Nostril deformity and uneven size
- Respiratory obstruction
- Difficulty in cleaning the nostrils
Surgical advantages
-
It is conducive to reducing the frontal width and visual area of the nasal tip.
-
It is able to effectively change the width and shape of the ala nasi, conforming to the perfect ratio.
-
It is able to simultaneously reduce the area of the exposed nostrils.
-
It is able to fixate the size and position of the nostrils, which do not flare up while laughing.
Surgical drawbacks/span>
-
Inner rim resection is unable to effectively reduce the size and exposed area of the nostrils.
-
Alar base may leave scars.
-
Excessive reduction may result in alar or nostril deformity.
-
Reversibility is relatively low.