Lateral Canthoplasty / Canthopexy
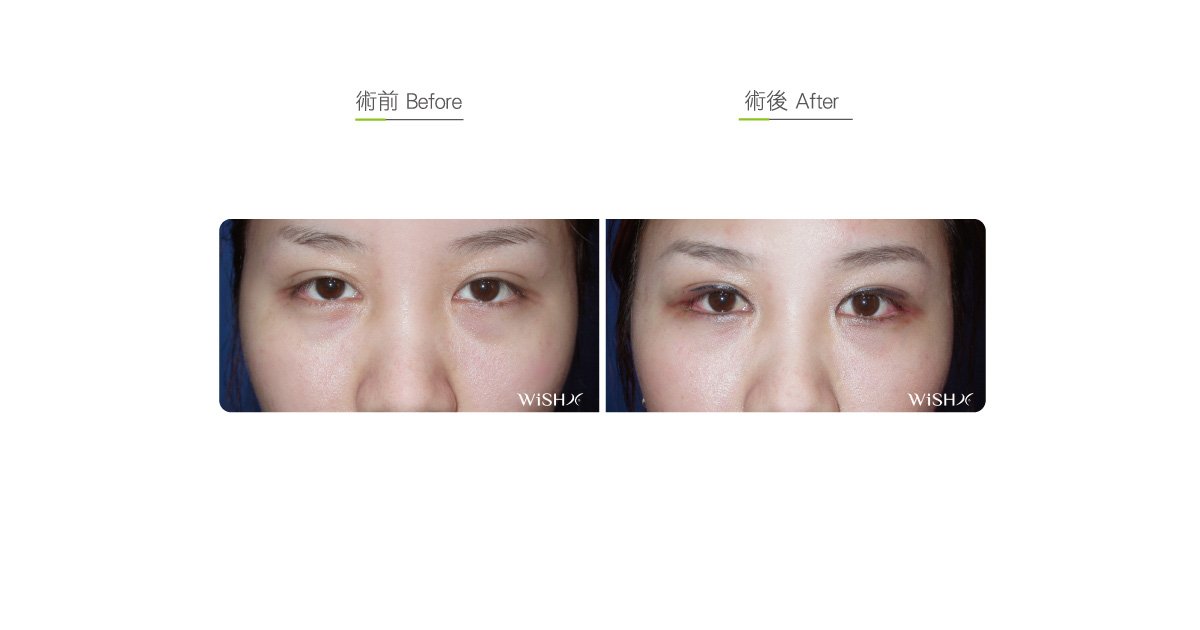
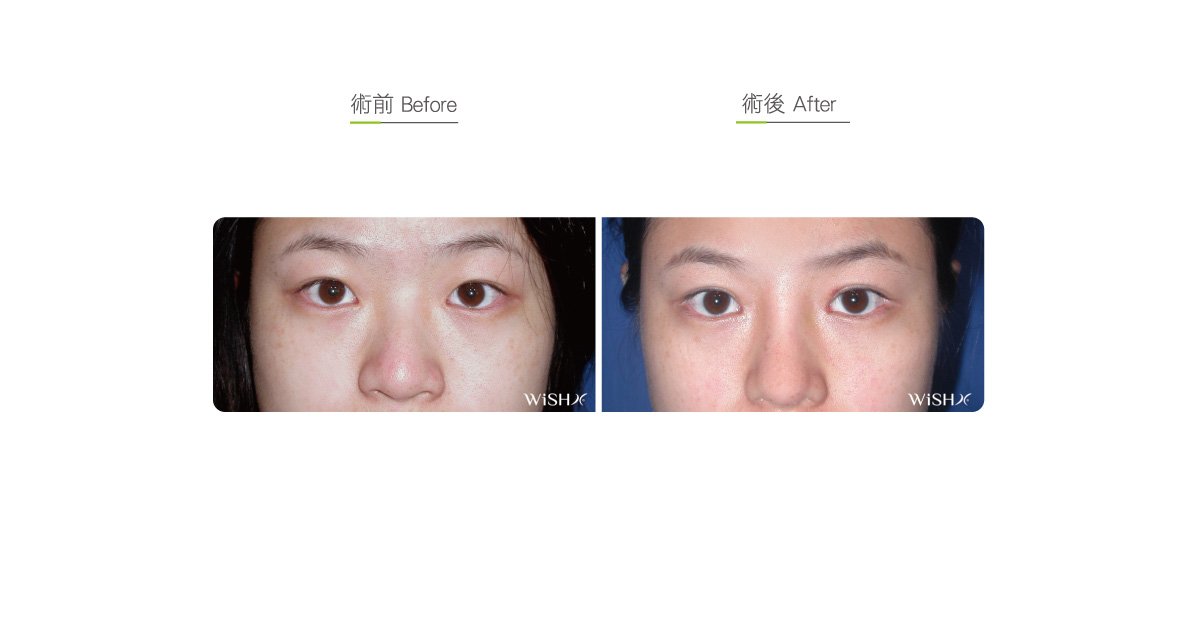
Compared with double eyelid or combined medial canthoplasty, lateral canthoplasty is unassociated with the shape or patterns of double eyelid folds and is a relatively independent surgical option. It is mainly used to dissect the connection between the superior and inferior eyelids at the lateral canthus (outer corner of the eye) and extends to the lateral side of the eyeball;, which it not only excises the redundant skin covering the lateral canthus but also increases the exposure of the white eye to achieve the effects of eyeball enlargement and elongation. The surgical incision is located at the margin of the superior and inferior eyelash skinsmargins, so the scar is less visible. However, because the wound suture sometimes stimulates the eyeball cornea, the patient’s eyeballs show temporary swelling and irritations when the stitches have not been removed within 1 week postoperatively. Moreover, the dissection site of the lateral canthus does not have eyelashes growing there and might present temporarily redness, stimulus, and other allergic symptoms temporarily. Therefore, Dr. Chuang suggests that patients willing to undergo lateral canthoplasty should consider its side effects and the recovery time before making a decision.
Besides enlarging the eyes, lateral canthoplasty rectifies the defects of congenital eye shapes like medial canthoplasty. For example, for patients with almond or slanted eyes or upward lifted medial lateral canthus (tropia), the physician adjusts the dissection angle of the lateral canthus to pull the whole lower eyelid medial canthus to the horizontal line, which improves the problem of excess inferior coverage at the lateral canthus. In addition, for some patients desiring semi-circular or big round eyes like a doll, Dr. Chuangthe physician excises the inferior eyelid skin along with lateral canthoplasty, which pulls the inferior eyelid horizontal line to a position parallel to the medial canthus, creating an eye shape required by the patient. For some young patients having congenitally low eyebrow bones resulting in pseudo ptosis of the lateral canthus, lateral canthoplasty is also utilized for partial eye shape correction.
Traditional lateral canthoplasty horizontally cuts the lateral canthus and then makes a simpledirect ssimple stitching directly on the superior and inferior eyelid wounds. This method is unable to achieve substantial elongation and but causes lateral canthus retraction due to scar hyperplasia, so the successful ratesatisfaction is was low in the past. Dr. Chuang utilizes the innovative V-Y advancement flap to perform surgery for lateral canthoplasty; hence, it is also called lateral canthopexy. Along with lateral horizontal pulling and extension of the lateral canthus, it requires releasing and dissecting the deep medial canthal ligaments and then fixating and stitching the repositioned medial canthus to the periosteum and ligament close to the lateral side of the eye socket, before partial skin resection and stitching at the defective parts of the superior and inferior eyelids. Its advantages are stable postoperative results that are less likely to retract and distinct enlargement (at most 3–4 mm); the drawbacks are the complex nature with long surgical procedures, relatively slow postoperative recovery, and occasional exposure of red flesh.
Dr. Chuang warns that the following patients may be unable to undergo lateral canthoplasty:
- Those having more white eyeballs at the lateral side than at the medial side.
- Those showing a tendency of inferior eyelid extropionversion or laxity (pupils at the superior position)
- Those who may have concerns of eyelash inversion or loss in at the dissection area
- Those with chronic or acute eye diseases who are unable to tolerate postoperative temporary stimulus to the conjunctiva or cornea postoperatively
- Those whose skin at the lateral canthus has already shown distinct laxity or sagging
Lateral canthoplasty
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: Close the superior and inferior eyelid margins at the lateral canthus
- Recovery: 7–10 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Avoid smoking, alcohol, and irritating foods for 1 month postoperatively, and do not wear contact lens.
- Avoid rubbing the eyes and contact with dust and dirty water for 3 months postoperatively.
Ideal candidates
- Patients with exceedingly small, round, and short eyes (like a copper bell)
- Those with congenital lateralmedial canthus upward slanting that leads to a distinct almond or Phoenix eye
- Those with normal eye shape conditions but desiring extreme enlargement of the eyes
- Those with congenital eye drooping (splayed eyes) but having normal eyelid skin at the lateral canthus and no laxity
Potential complications
- Scar adhesion
- Lateral canthus retraction
- Eyelash defect
- Cornea/conjunctiva scraping (temporary)
- Lateral canthus redness
Surgical advantages
-
It horizontally extends the lateral canthus to the lateral side to enlarge the eyes.
-
It adjusts the visual area of black eyeball and white eyeball close to the 1:1 golden ratio.
-
It modifies eye shape defects such as congenital heterotopia or Phoenix eye.
-
Lateral canthus elongation helps modify the misconception of the drooping of congenitally splayed eyes.
-
It achieves extreme eye enlargement if conducted along with medial canthoplasty.
Surgical drawbacks
-
Temporary cornea or conjunctiva redness, sw or swelling or irritation may occur after the operation (approximately 1 week).
-
The lLateral canthus may show prolonged redness or irritable symptoms.
-
No eyelash will grow at the dissected eyelids.
-
Incisions may show retraction or scar adhesion.
-
Partial eyelashes at the lateral canthus may demonstrate malposition or inversion.