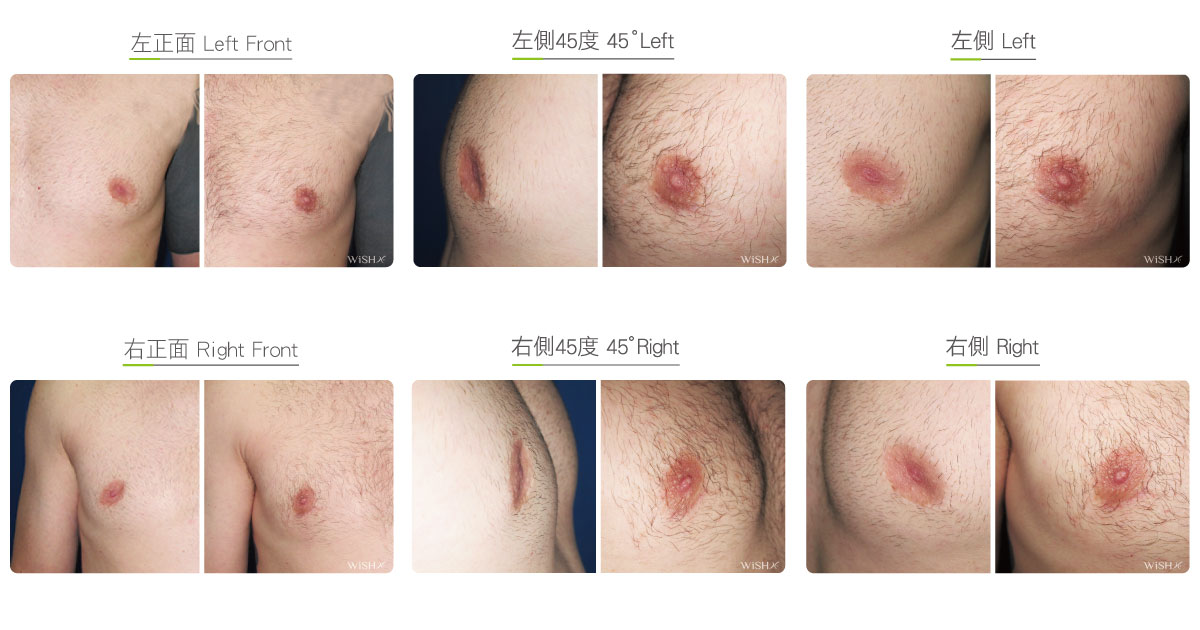
Retracted Areolar Correction
Concave areolae are rare in clinical settings. Some common causes include internal scar contracture caused by mastitis, secondary loosening and sinking of the nipple due to severe mammary gland atrophy, and scar adhesion from previous surgeries with periareolar incision (e.g., breast augmentation or mastectomy), with few cases caused by malignancy in the breast tissue. The method of correction depends on the severity of concavity. In general, there are two surgeries:
- Fat Transfer
If concave areola is caused by breast ptosis, sagging, or atrophy, then the quick and simple autologous fat transfer procedure can be performed to fill the loose space underneath the areola. This surgery is less invasive and has a short recovery period, but the fat can be reabsorbed and gradually disappear. It is commonly performed along with autologous fat transfer breast augmentation for added results.
- Dermal Fat Transplant
It is designed for severe concave areolae caused by scar adhesion from surgeries or mammary gland inflammations. Fat injection alone cannot improve this problem, and thus, thicker and tougher autologous dermal fat tissue from gluteal or inguinal fascia is used. The surgery first releases the scar at the site of adhesion, creates the loose space under the skin, and then, the complete fascial tissue harvested from the gluteal line or inguinal fold transplants to the subcutaneous space of scar site. This surgery has more evident and lasting results with a lower absorption rate (<15%), but it would leave an additional scar on the donor site. It also takes time for the areolar wound to heal.
Besides autologous tissue grafts, breast implants used in augmentation mammoplasty can also correct atrophic or concave areolae. Thus, many patients with ptotic or atrophic breasts will choose breast augmentation to improve the problem of concave or loose areolae at the same time.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Type of incision: periareolar incision and near the gluteal or inguinal fold (for fascia harvest)
- Recovery: Immediate
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery
- Pressing or rubbing of the areolar area should be avoided for 1 month postoperatively.
- Smoking, alcohol consumption, and wearing tight clothes that could compress the areola and nipples should be avoided for 3 months postoperatively.
Ideal candidates
- Those with mammary gland atrophy and concave areola due to multiple pregnancies or breastfeeding.
- Those with wrinkled or loose areolae due to breast ptosis.
- Those with concave areolae due to a previous surgery with areolar incision.
- Those with concave areolae due to a contracture caused by mammary gland inflammation.
Possible complications
- Relapsed concavity
- Incomplete correction
Surgical advantages
-
Quick and evident results.
-
Restores the normal appearance of areolar skin.
-
Improves nipple or areolar deformation caused by scar adhesion.
Surgical drawbacks
-
Concavity may relapse.
-
Uncertainties of autologous fat transfer such as absorption.
-
Additional scar on the buttock or inguinal area if dermal fat tissue is used.