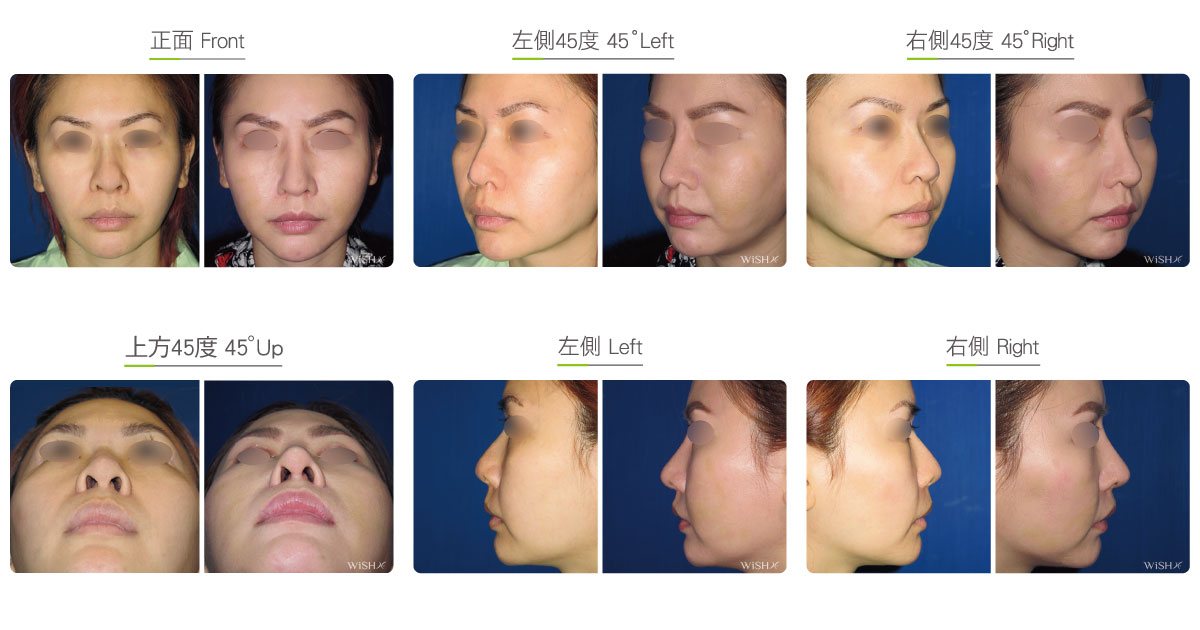
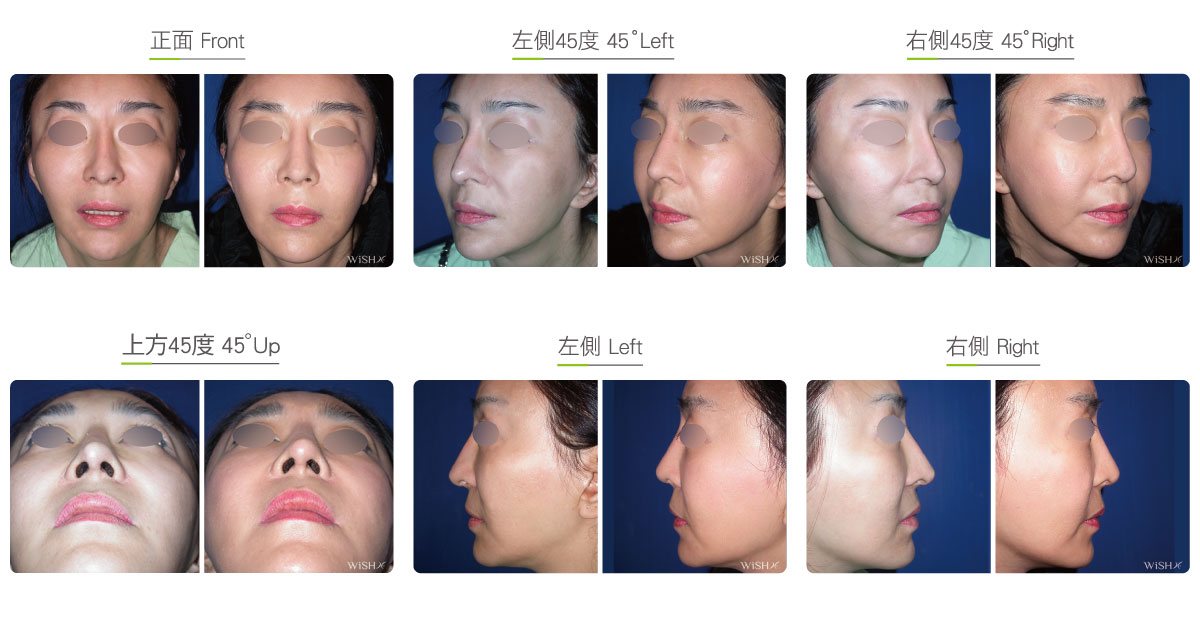
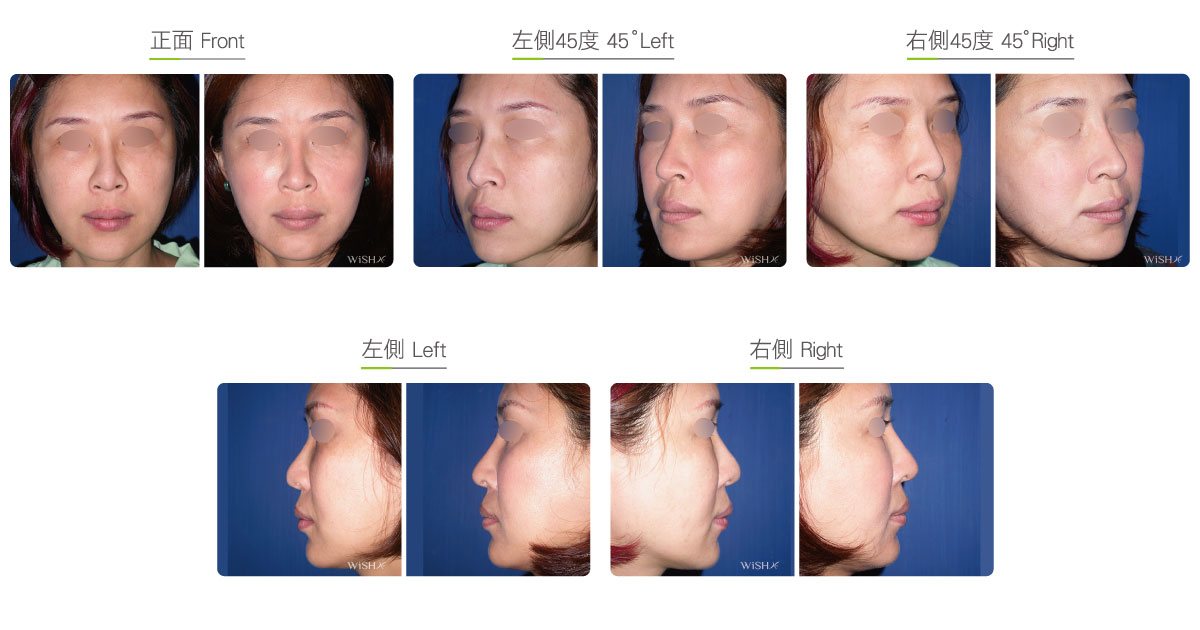
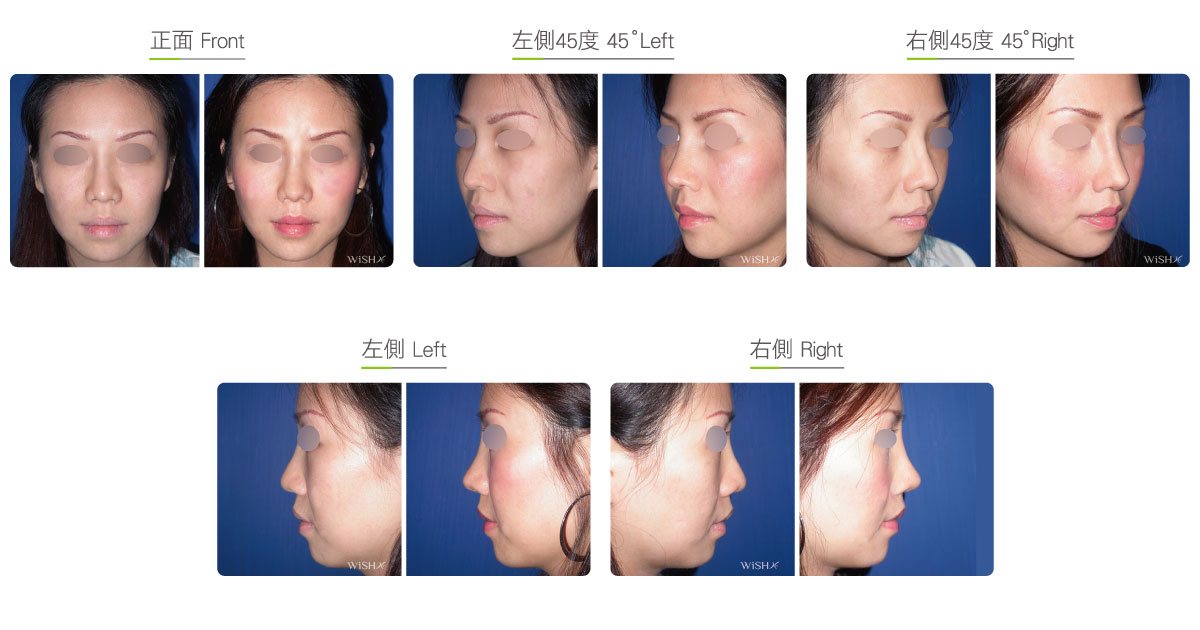
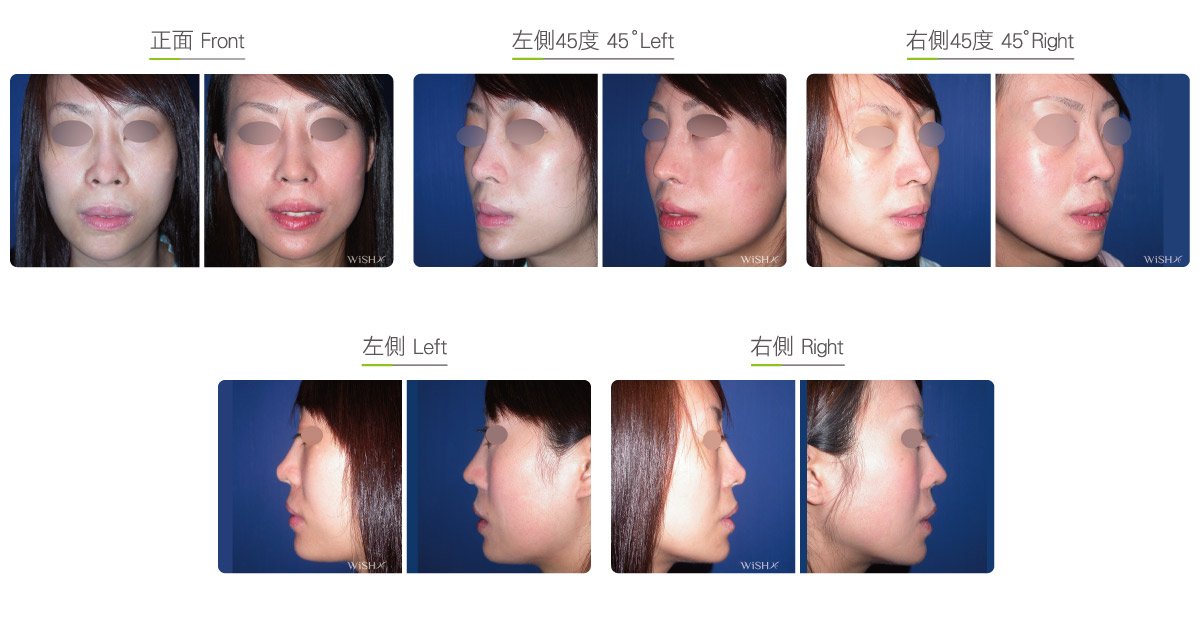
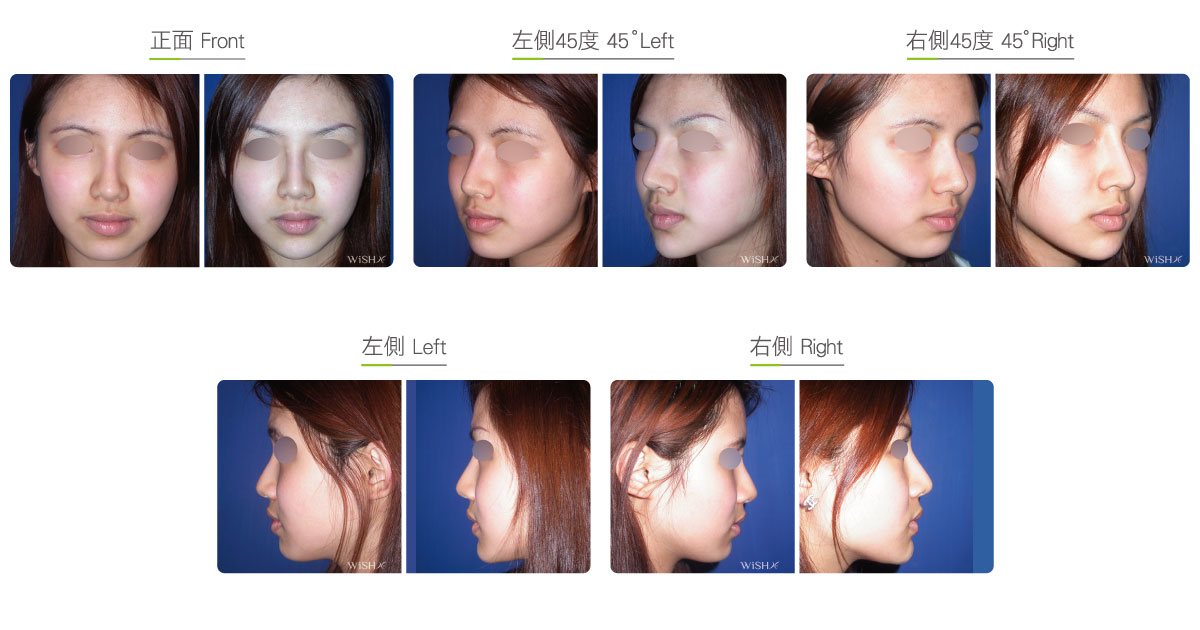
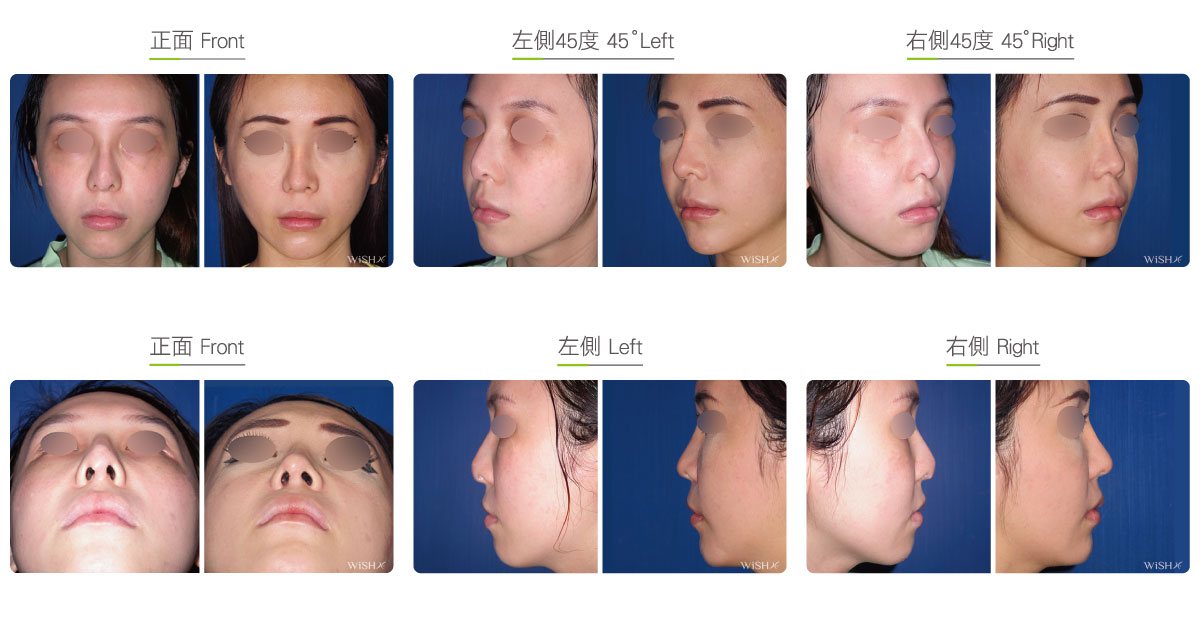
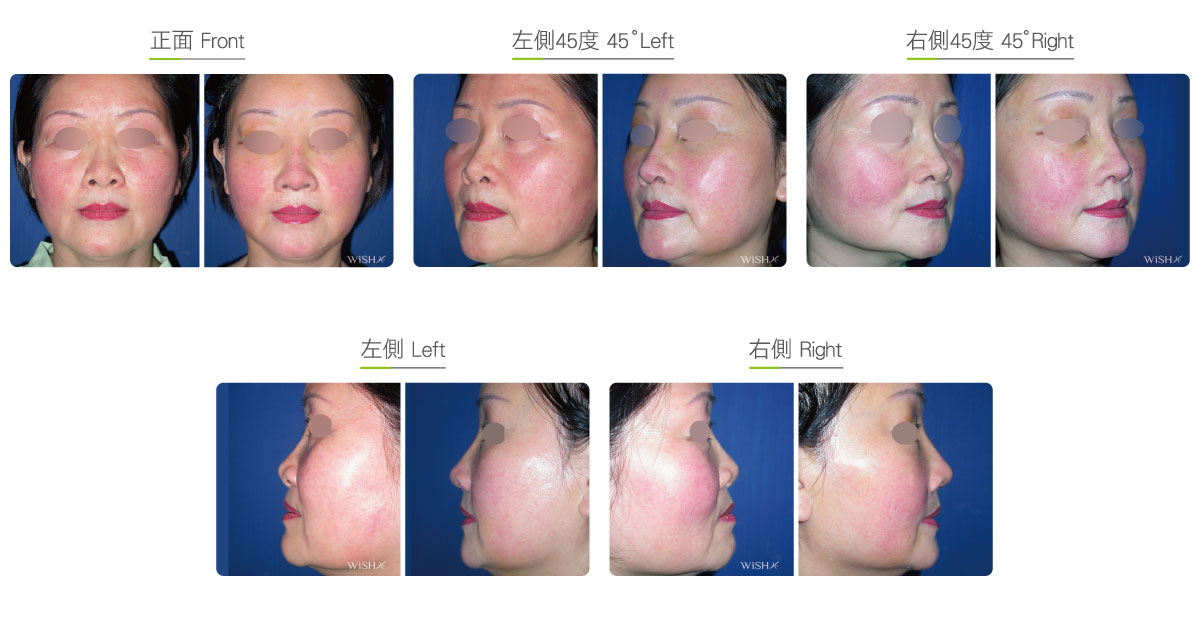
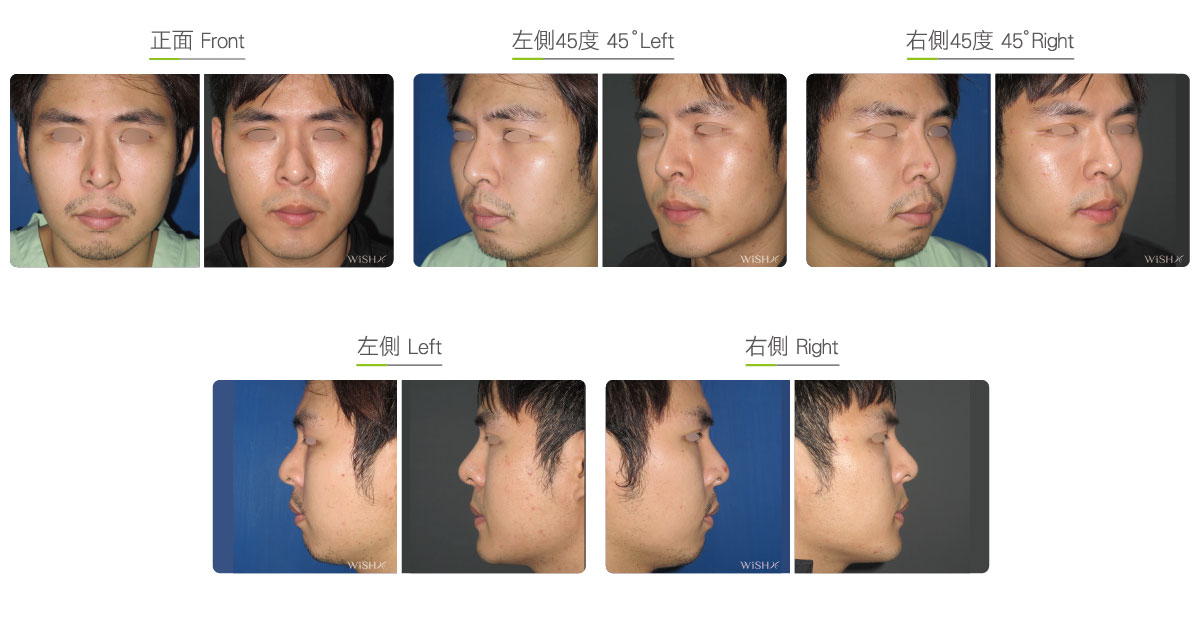
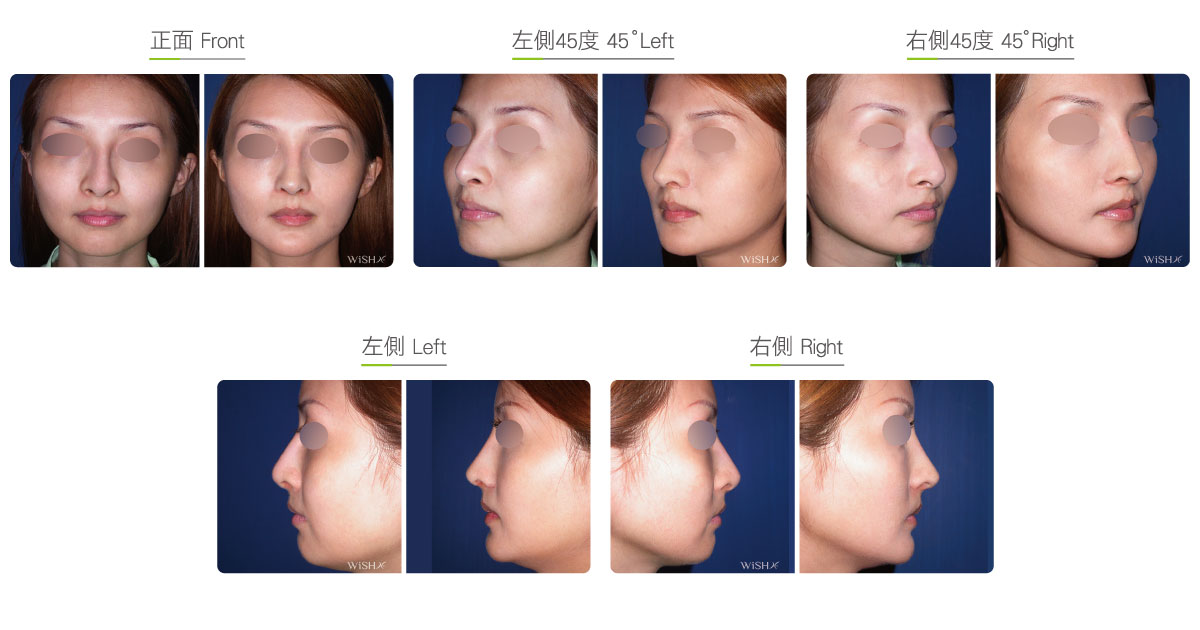
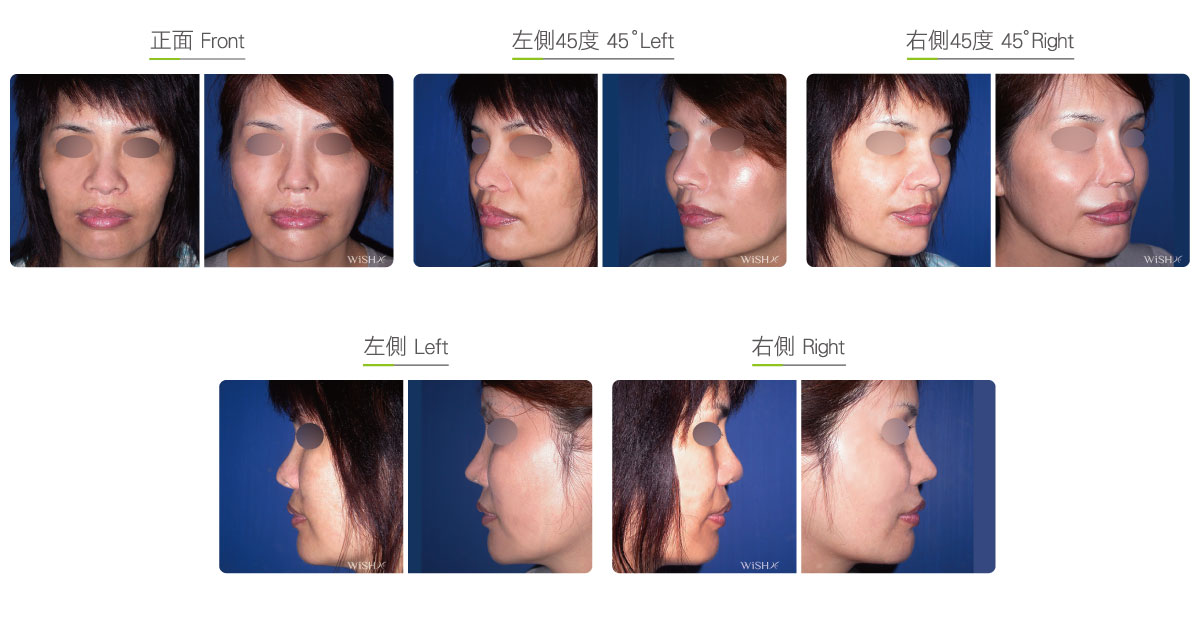
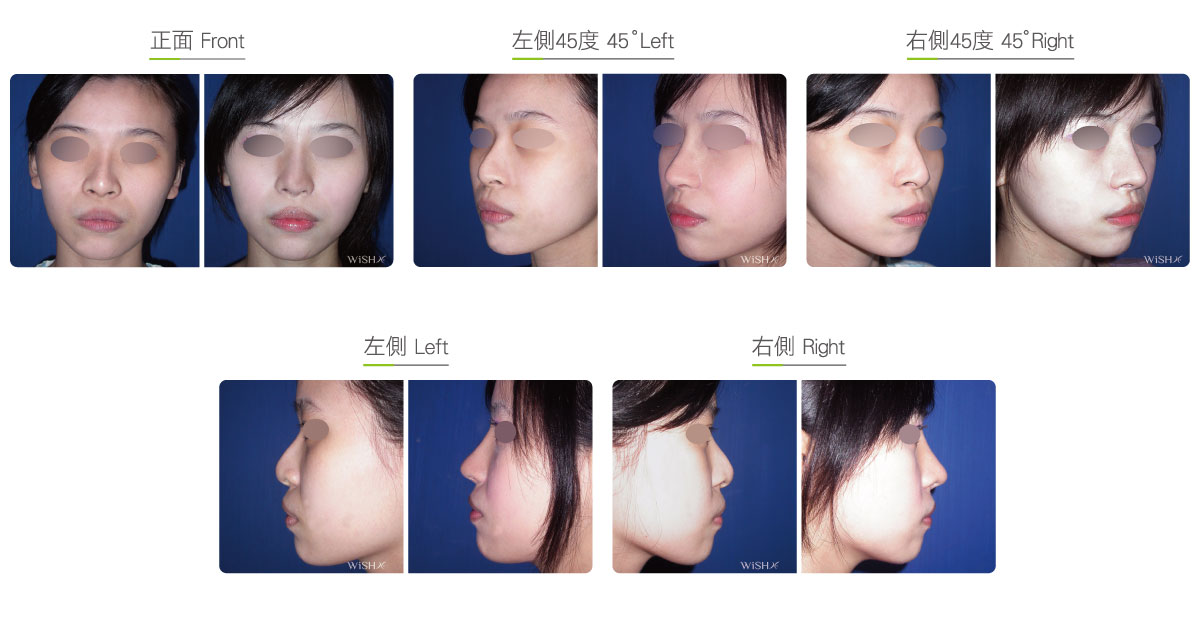
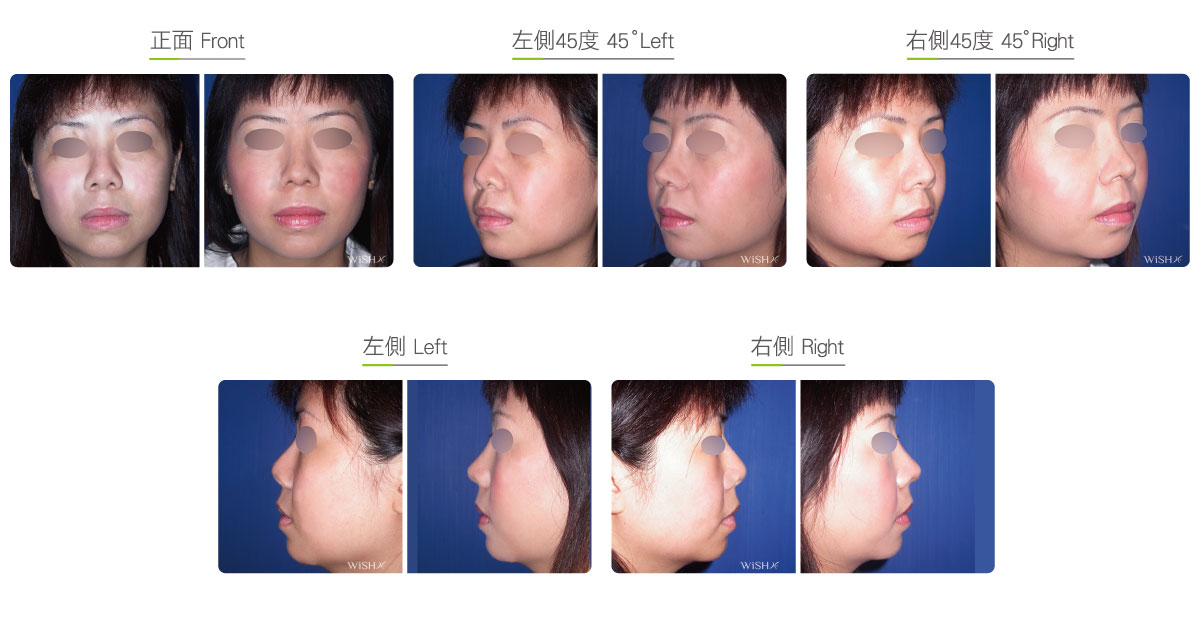
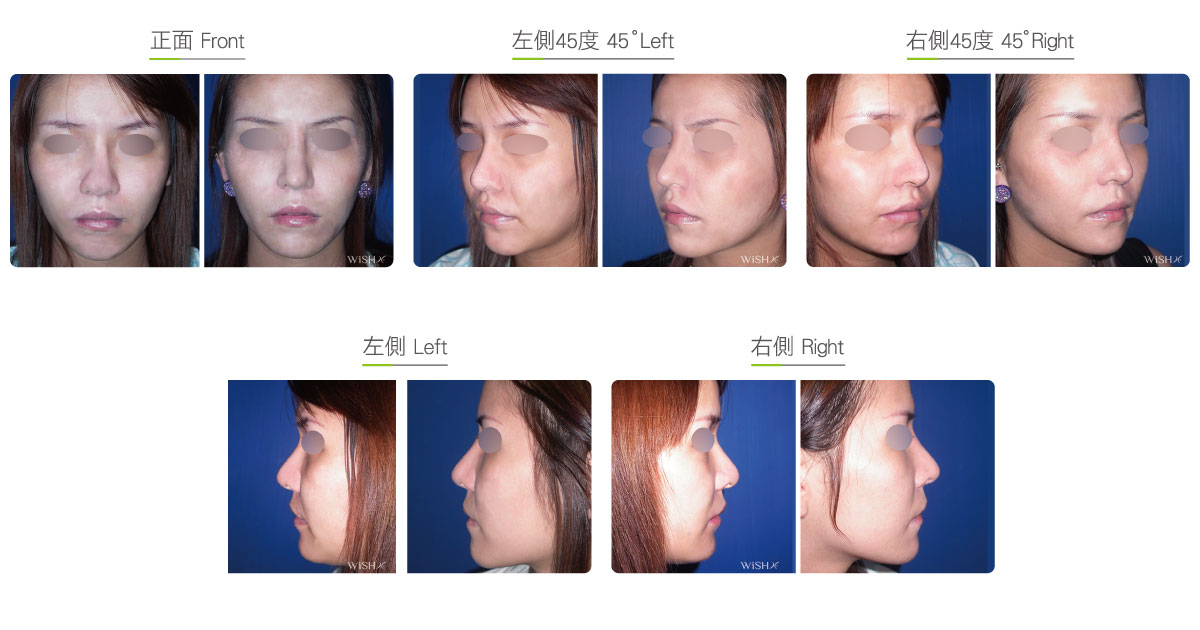
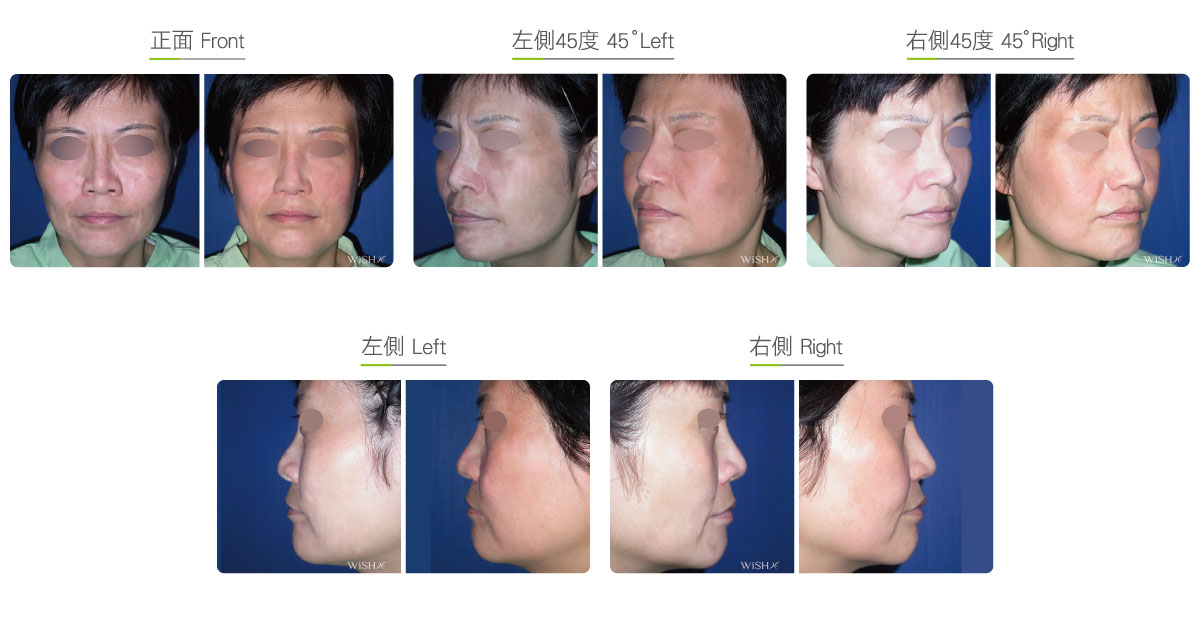
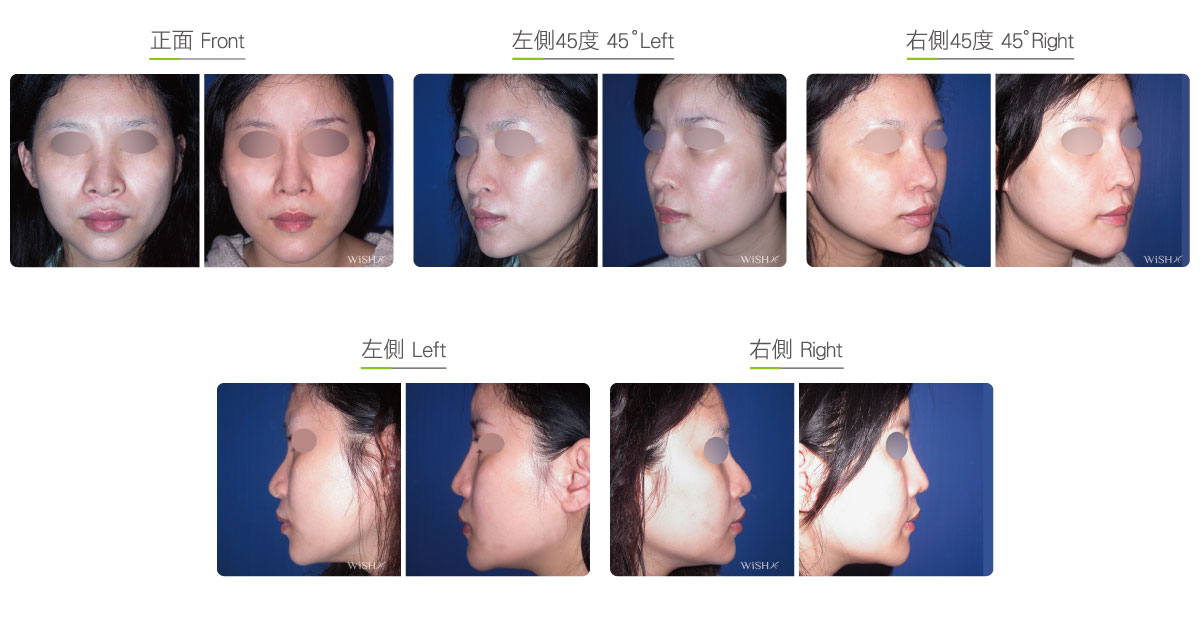
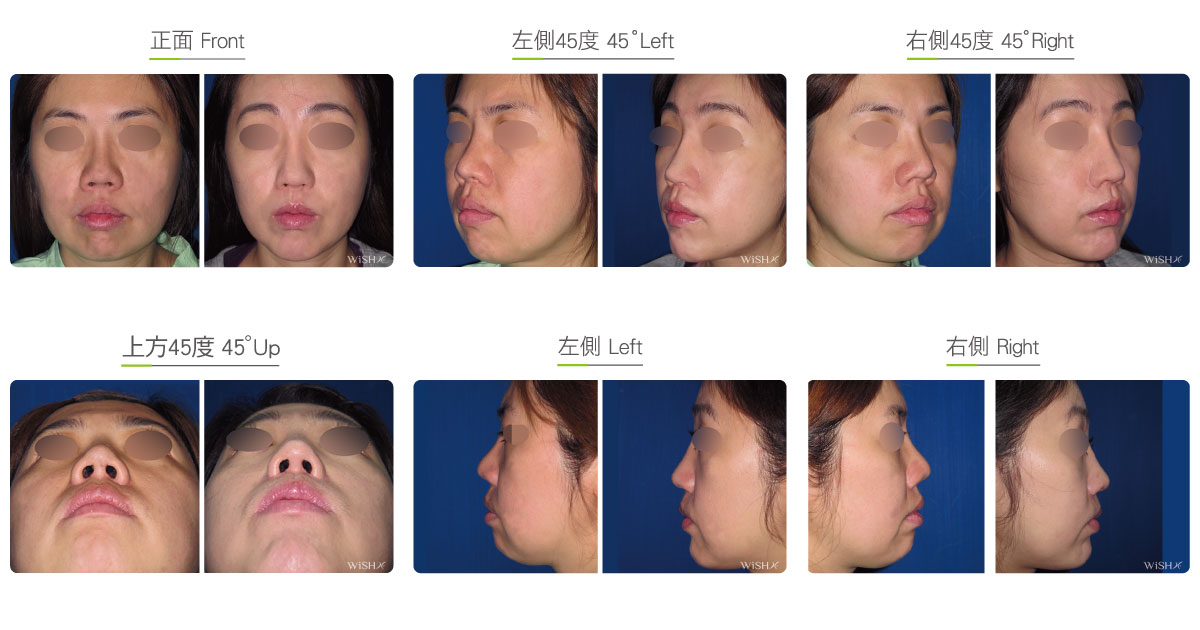
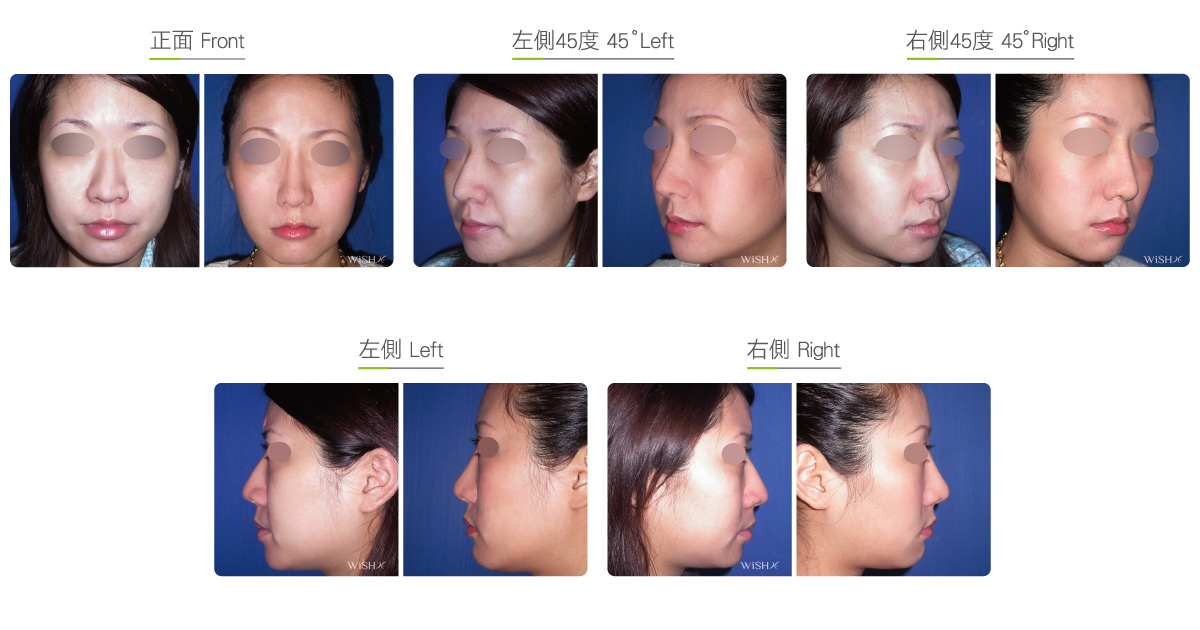
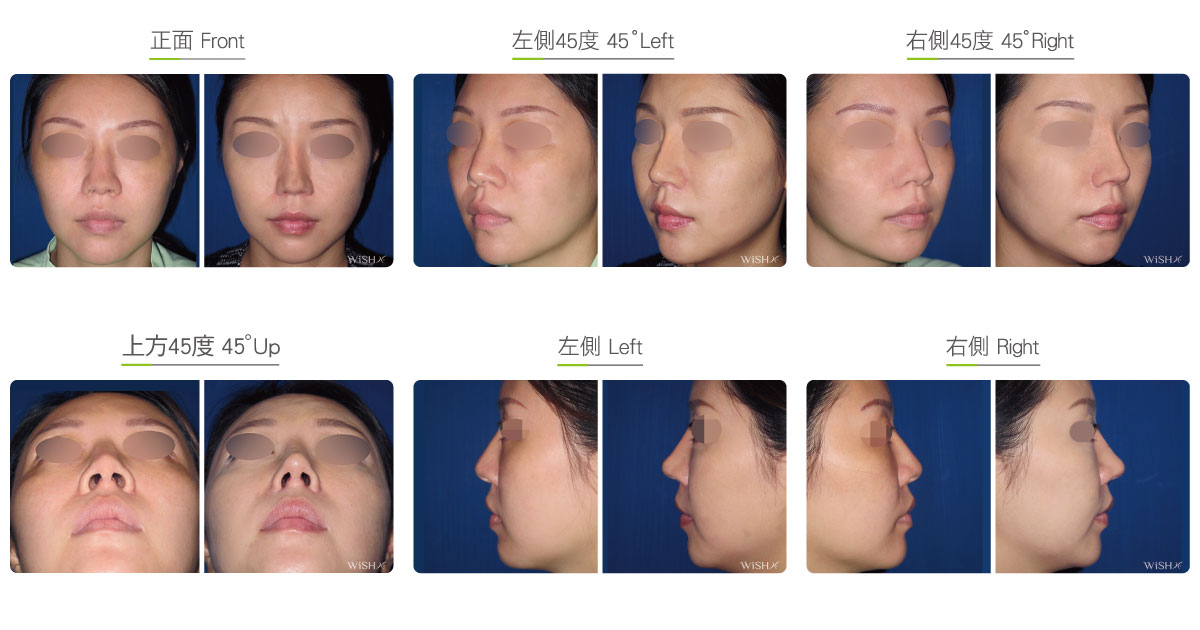
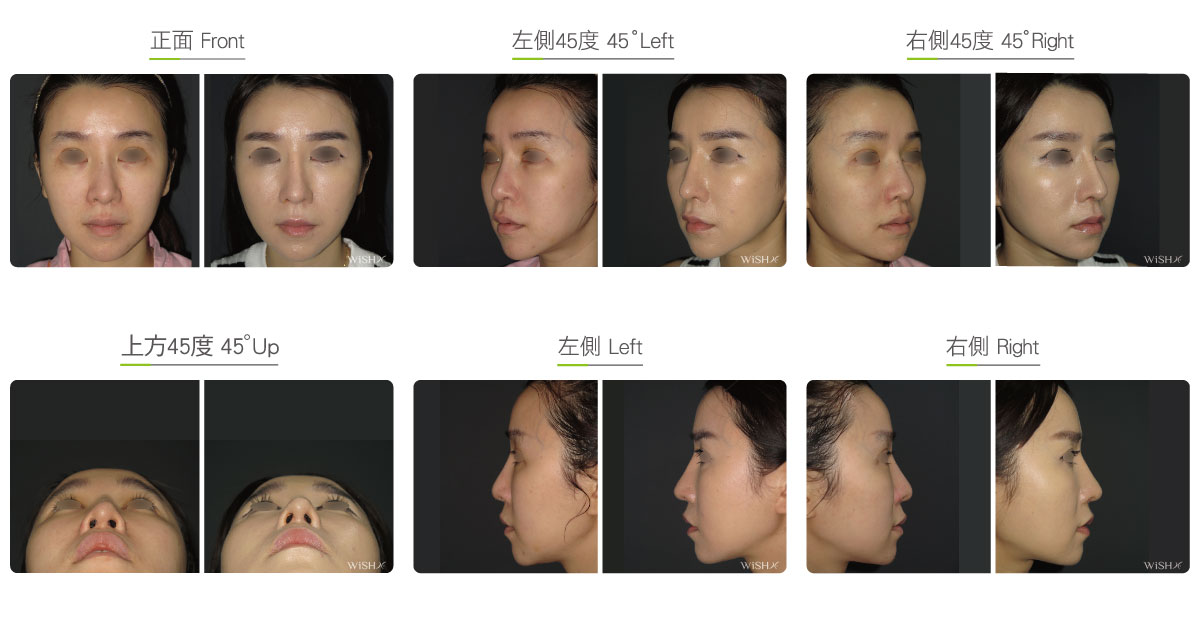
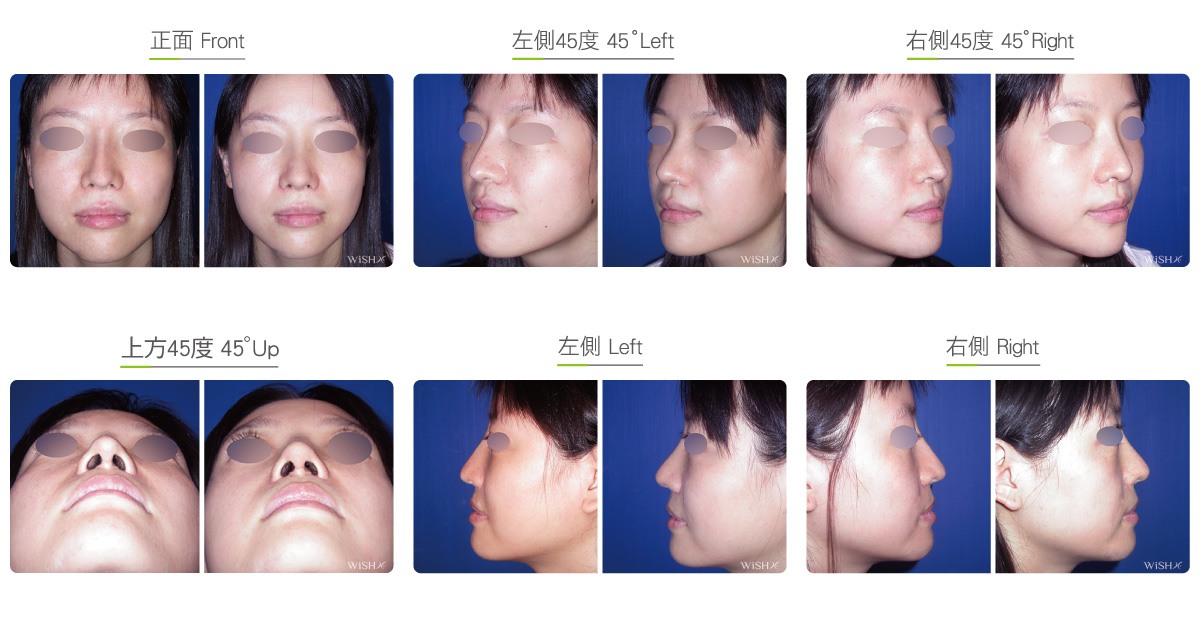
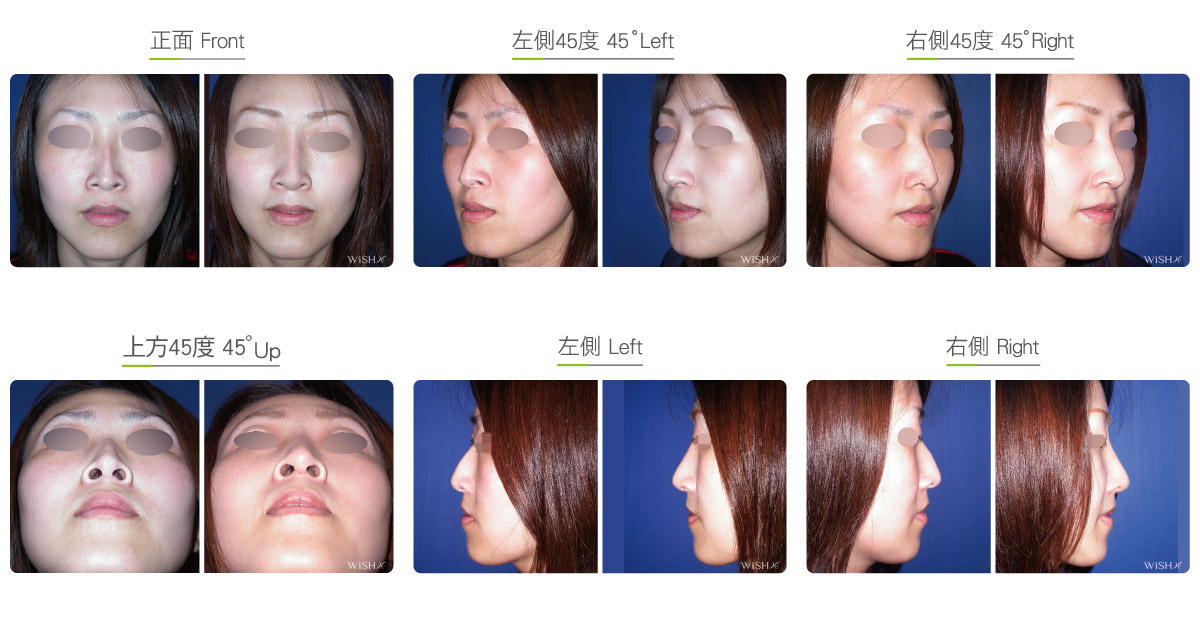
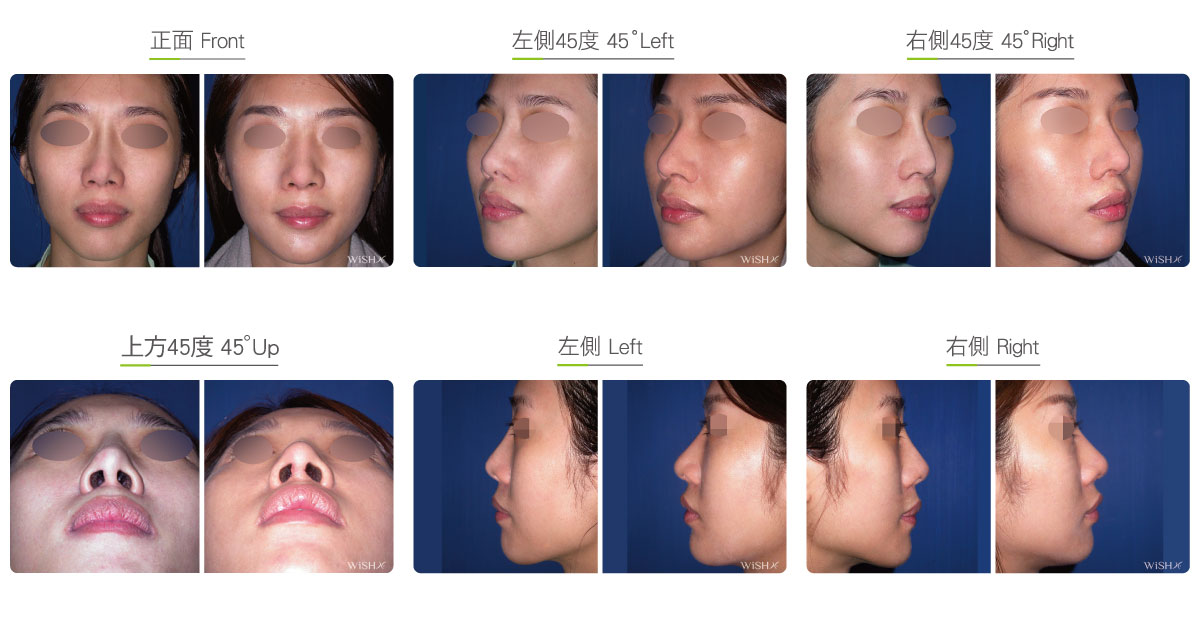
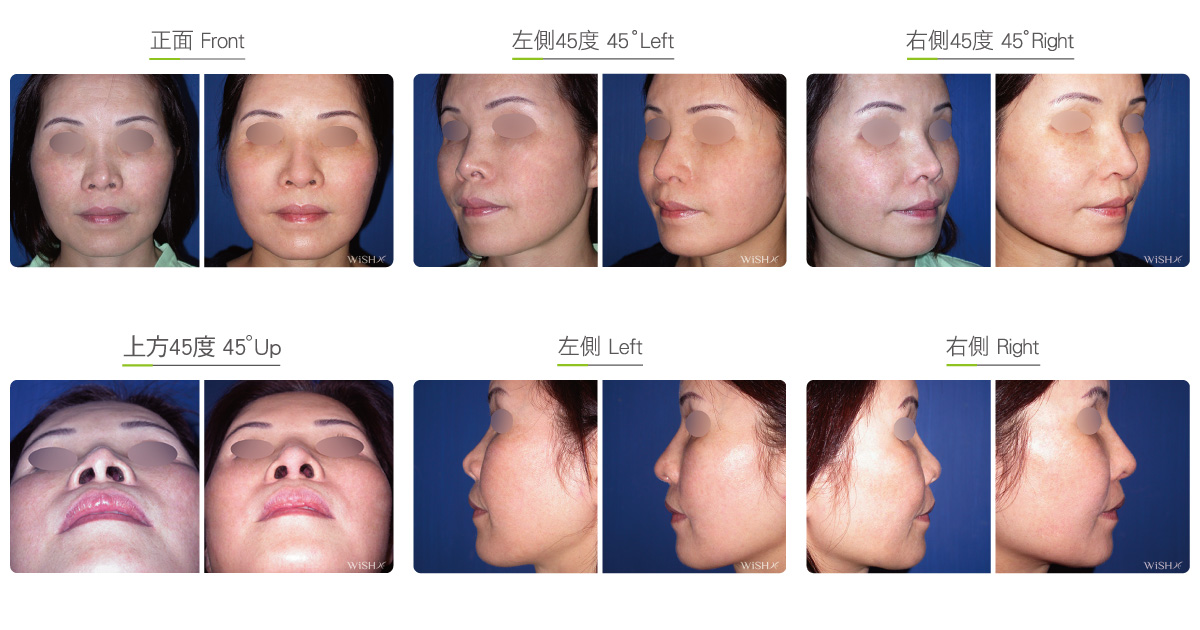
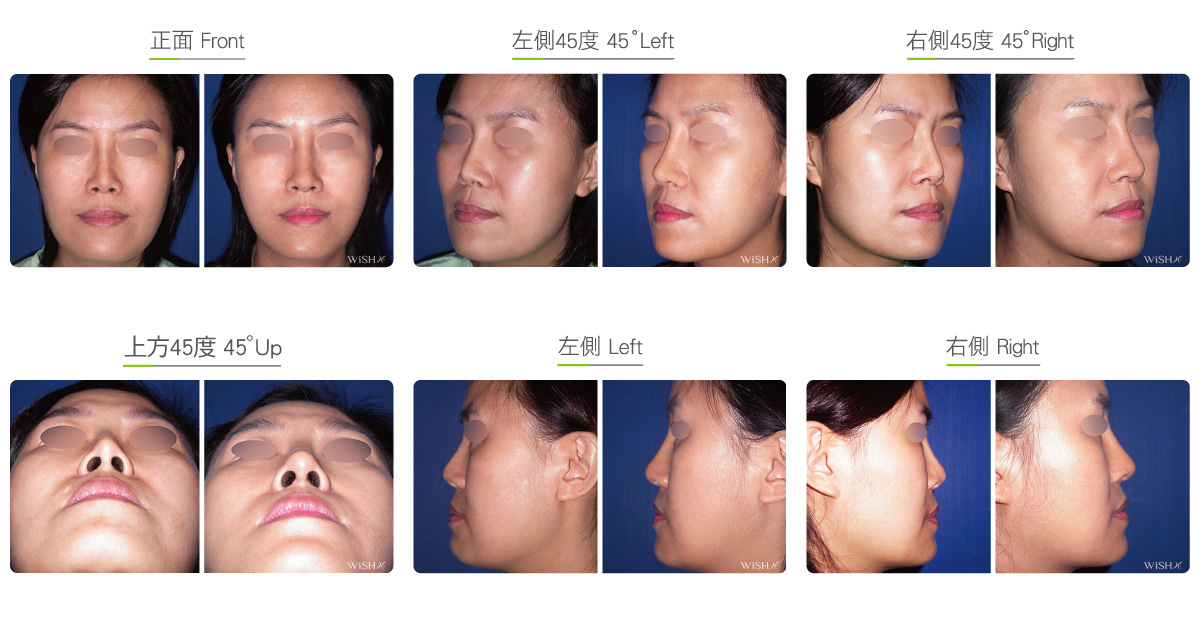
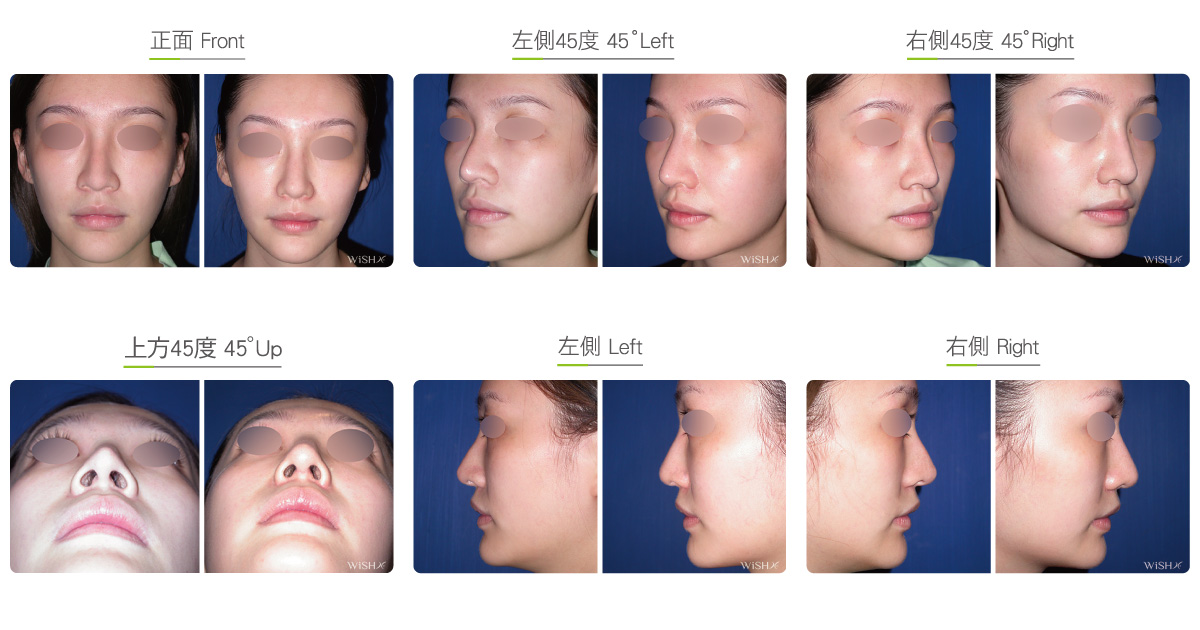
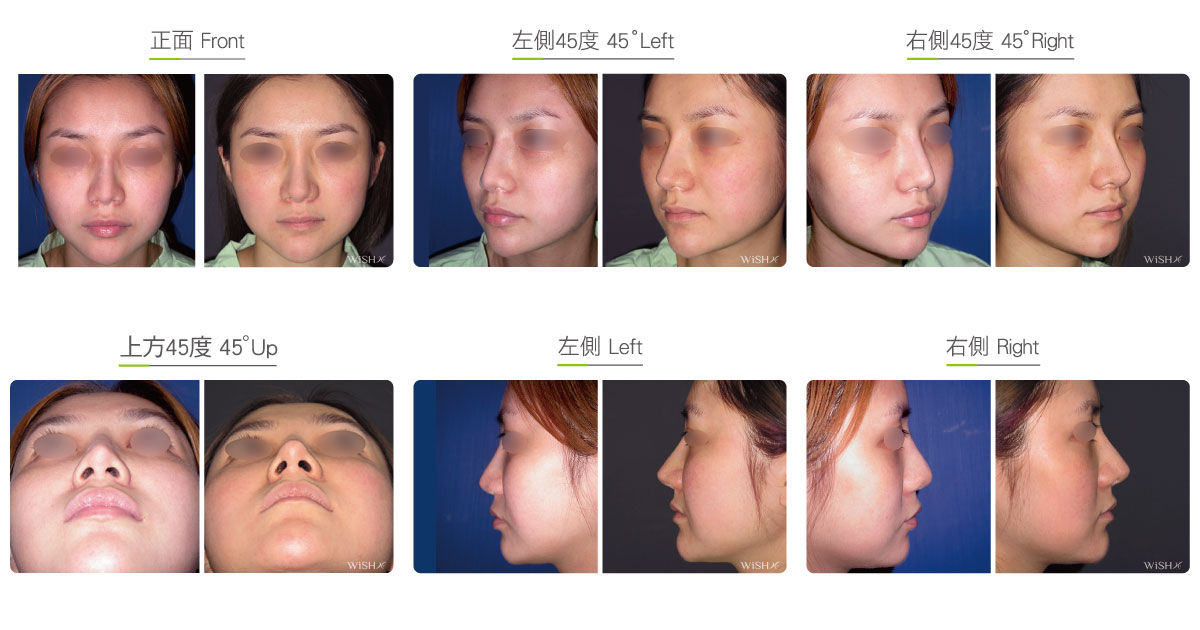
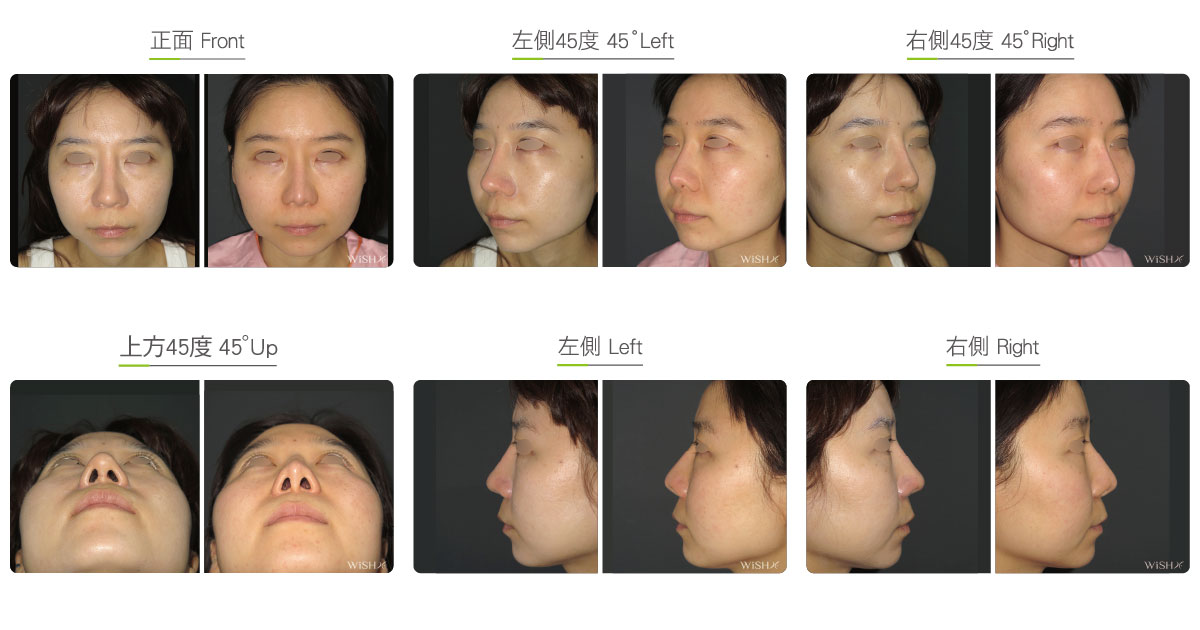
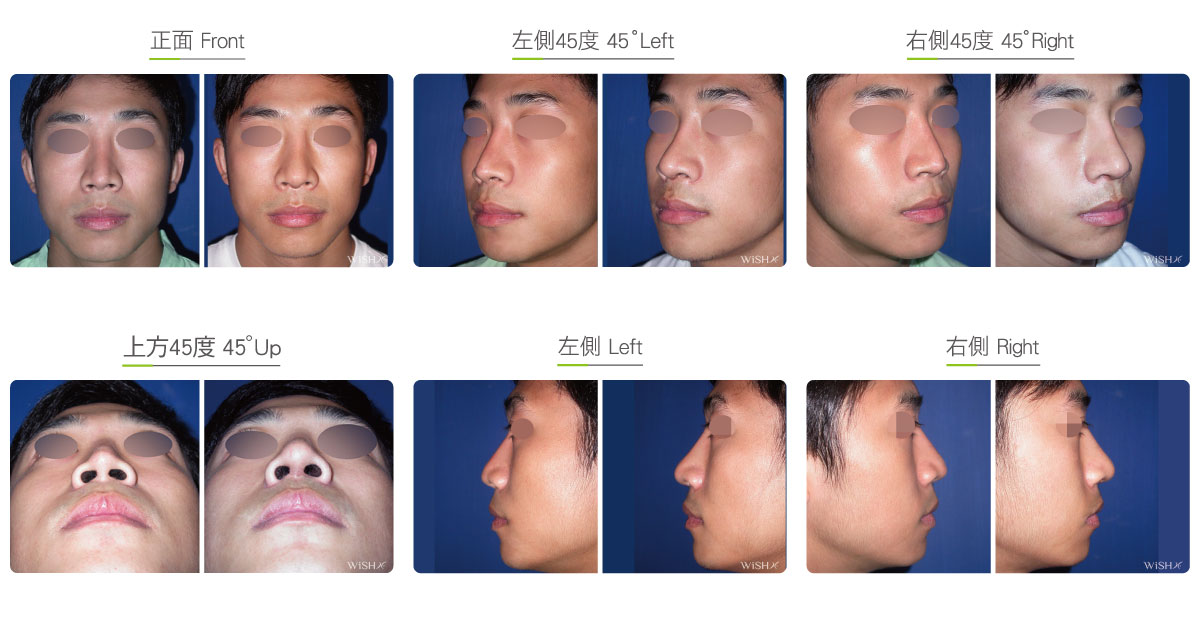
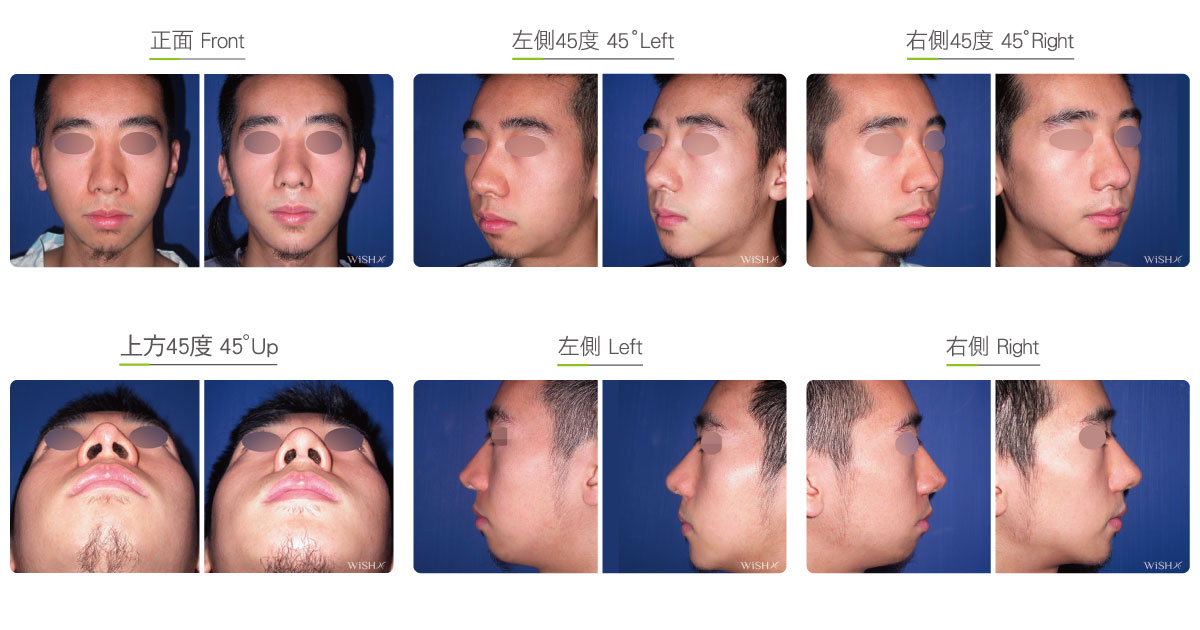
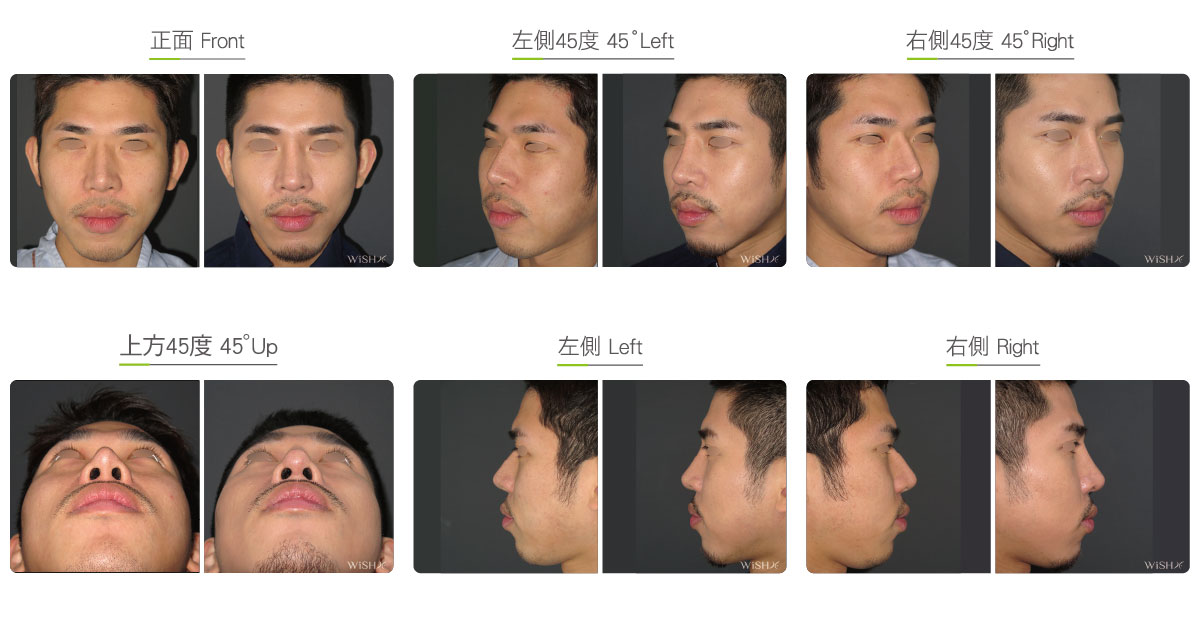
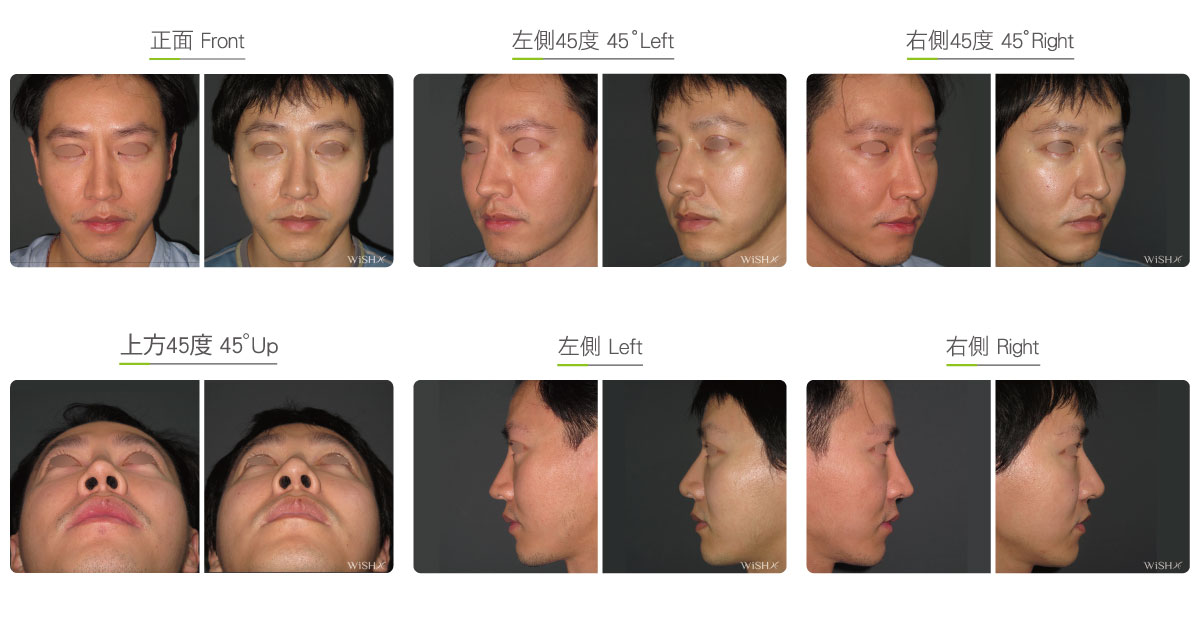
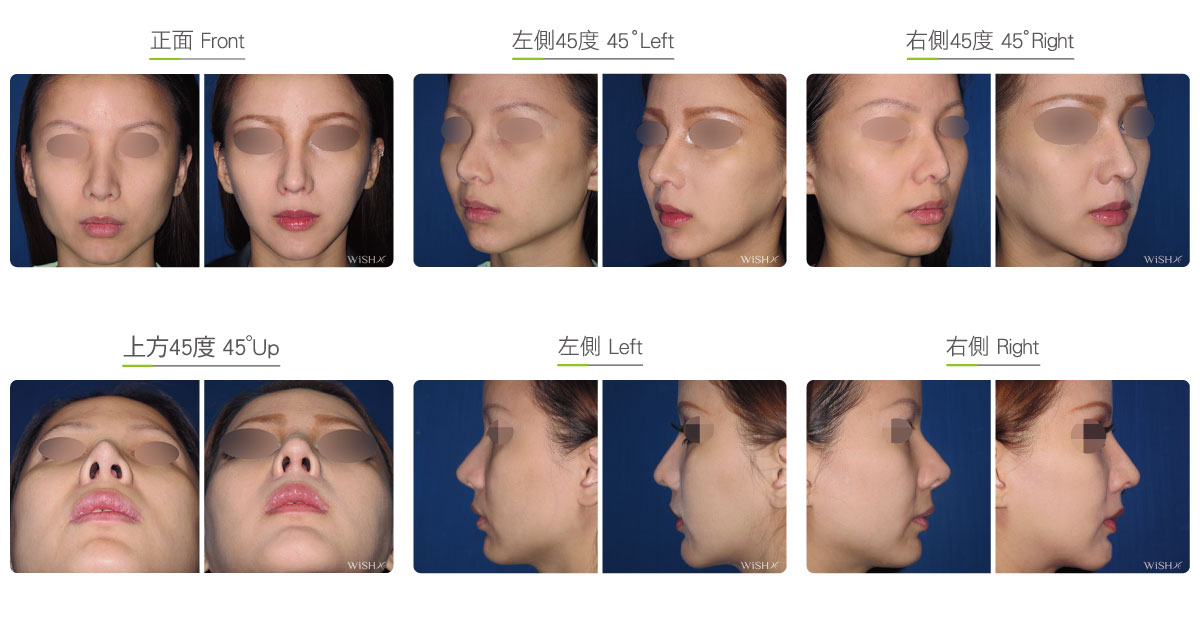
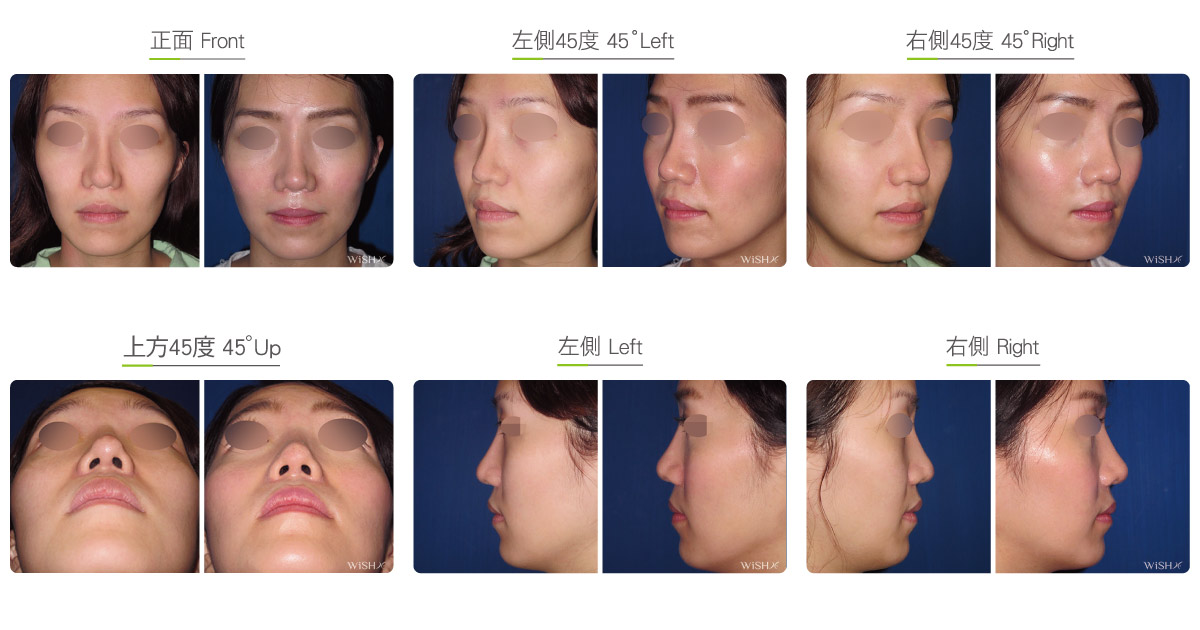
Secondary open rhinoplasty
Rhinoplasty is one of the most subjective plastic surgeries. Considering the differences in patients’ expectations and requirements as well as the physician’s esthetic value, the results sometimes fall short of expectation or satisfaction; therefore, the unsatisfied patients want to reconstruct or remodel the noses. Nevertheless, secondary surgery is more complex than the primary operation, which should not only redress the defects of the original surgery but also fulfill the patient’s high expectations. Therefore, the highly customized open rhinoplasty will be employed to achieve comprehensive improvements.
Revision open rhinoplasty is identical to general open rhinoplasty, but surgical conditions and complexity greatly differ in light of the patient’s objectives and prior problems. It is performed by detaching the nasal skin first, removing the nasal implant placed by previous surgery via a columellar incision and resecting intranasal scars and capsules before emplacing a brand new implant along with the harvested nasal septal or auricular cartilage to fully reconstruct the nasal tip. However, the more times the revision is performed, the more fibrotic the intranasal tissues will become. In such cases the surgical improvement would be confined, and the incidence of infection will increase. Therefore, Dr. Chuang recommends that patients willing to undergo secondary rhinoplasty should take into full consideration their real requirements and communicate well with the physician before the operation to achieve expected results in one surgery as well as to avoid the risks of other revisions. In addition, for patients whose implant is removed due to infection from the prior surgery, Dr. Chuang advises them to wait for 6–12 months before undergoing rhinoplasty again to ensure the safety of the secondary operation.
Dr. Chuang highlights the following aspects in revision open rhinoplasty:
- Replacement of nasal implant
The size and model of the nasal implant affects the naturalness and definition of the nasal bridge. Because early silicone implants frequently induce obvious defects such as an excessively narrow bridge or a reflective bridge shadow, the latest Sili-Tex (Chimera) composite nasal implant or Gore-Tex material will be ideally considered for revision surgery. Such materials not only address the contracture of the capsule or shifting of the silicone implant but also offer multiple sizes for the adjustment of the nasal bridge height and lower the risks of infection or foreign body reaction from revision surgery. - Reconstruction of nasal tip cartilage
Generally, patients willing to undergo revision rhinoplasty are mostly unsatisfied with the shape or size of the nasal tip, so the septal cartilage or combined auricular cartilage should be harvested to sculpt the nasal tip. The cartilage emplaced is more than that in the prior surgery to reconstruct the nasal tip triangle by the replacement of abundant cartilage, thus achieving the results of the slightly upward slanting of the supra-tip angle, elongation or reduction of the nasal tip, and extension of the columella strut. - Nasal fat padding
The nasal tip skin in some patients becomes thin or shows white spots due to the prolonged friction or compression of the nasal implant, which aggravates the risks of secondary surgeries. In consideration of the naturalness and durability of the thin skin patients, Dr. Chuang recommends patients to undergo additional autologous gluteal fascial transplantation at the nasal tip to flesh up the fat tissue, thus ensuring the long-term results of revision surgery and avoiding prosthesis protrusion, pointed tip deformity, and other rare complications. - Alar and nostril reduction
Early single nasal implant emplacement only improves the height of the nasal bridge but usually ignores the significance of the ratio between the alar and nostril widths and the nasal tip. However, based on the principle of open rhinoplasty, nasal tip sculpting usually needs to be concurrently performed with the reduction of the ala nasi and nostrils to achieve the perfect “pyramidal” tip shape. Therefore, alar and nostril reduction should frequently be taken into account in revision rhinoplasty to obtain the best result. - Autologous or homologous costal cartilage graft
A few patients who get an infection or foreign body reaction to the artificial nasal implant or in whom several prostheses fail to be implemented need to consider undergoing revision rhinoplasty with a fully autologous or homologous costal cartilage. As a part of the human body, the costal cartilage does not induce rejection or infection, effectively lowering the incidence of infections. Moreover, for patients who suffer from nasal tip deformity or contracture due to multiple failed revisions, autologous ribs provide abundant materials to reconstruct the entire nasal tips, which decrease the recurrence of nasal tip contracture or deformity due to insufficient support of tip structures.


Aside from careful selection of nasal implant material, the surgery and esthetic sense of the surgeon are both essential to success of rhinoplasty.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia or general anesthesia (for nasal bone correction)
- Surgical incision: At the inferior margin of the nasal columella and inside the bilateral nostrils
- Recovery: 7 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Wear a tape or plate for 1 week postoperatively to stabilize the nasal bridge.
- Avoid smoking and alcohol and impacts to the nasal bridge for 3 months postoperatively, and clean the intranasal wound in the morning and evening every day.
- Try to avoid raw food, seafood, and irritating food or spices for 3 months postoperatively.
- Try to avoid dirty water (such as sea water, swimming pool water, sauna water, and hot springs) or close contact with pets and dust mites.
- Please visit a doctor immediately in case of flu after the operation.
Ideal candidates
- Patients with a loose, deviated, or shifted nasal bridge implant
- Those with a shrunken or deformed nasal tip due to capsular contracture of the silicone implant
- Those who show an excessively sharp tip or white spots at the nasal tip, which is pending on implant extrusion
- Those who have a foreign body reaction or chronic inflammation caused by a prior nasal implant
- Those who have unnatural signs such as an excessively sharp, thin, or high nose and dissatisfied result with the prior surgery
- Those who need revision surgery as the nasal implant was removed due to infection from the prior surgery
- Those who desire better results than those from the prior surgery
Potential complications
- Nasal tip stiffness
- Nasal obstruction
- Infection
- Foreign body reaction
- Poor wound healing
- Columellar scar
- Recurrent contracture or deformity
Surgical advantages
-
This surgery improves the subjective satisfaction of patients.
-
Revision open rhinoplasty highly customizes the nose shape expected by patients.
-
The augmentation of the nasal tip by the cartilage from different body parts (nasal septum, auricular cartilage, or costal cartilage) effectively alleviates the nasal tip contracture or deformity caused by the prior surgery.
-
The surgery reconstructs the contracted nose and restores its normal appearance.
Surgical drawbacks
-
The surgery takes a relatively long time, and the incidence of postoperative inflammation or infection is relatively high.
-
Multiple revision surgeries could also increase the risk of infections.
-
The nasal skin may become thin, sensitive, and reddish due to revision surgeries.
-
The nasal tip is relatively hard, and future motion may be limited.
-
Surgical costs may increase due to problems caused by the prior surgery.