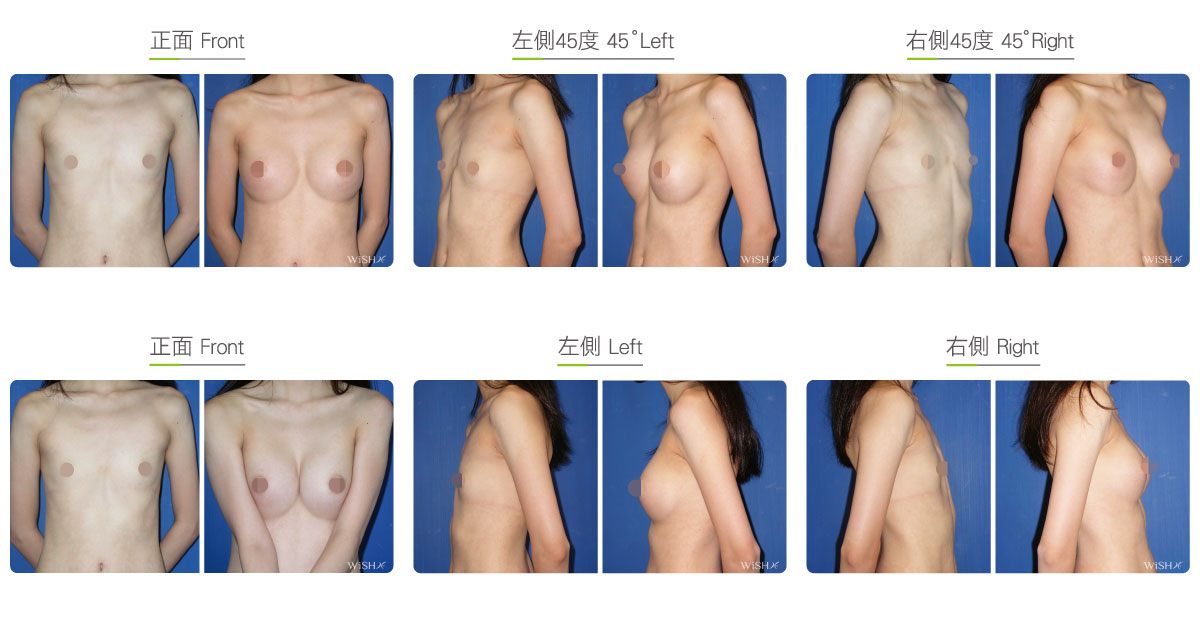
Asymmetric Breasts
Asymmetric breasts include two types of structural deformities. One refers to simple uneven breast tissue development with a normal sternum, e.g., asymmetric breasts. It is common among female breast augmentation patients and can be fixed by the placement of different sizes of implants. The other type results from asymmetric skeletal development, e.g., breast at different heights. The causes of the latter type of deformity are more complicated. For example, severe cases could be caused by Poland syndrome, which is characterized by the congenital underdevelopment of unilateral breasts or pectoralis. More commonly, the asymmetric development of the sternum is due to acquired factors such as scoliosis or poor postures during adolescence. These patients are characterized by evident height differences between the two sides of the ribs. In severe cases, even the breast midline is not aligned with the body axis; thus, a more thorough consideration is needed during evaluation and surgery. Patients with asymmetric chest have the following characteristics:
- Size difference of more than half a cup between the breasts
- Breast midline is not aligned with the body axis
- Evident height differences in bilateral breast or nipple positions
- Substantially concave sternum or ribs on one side
- Frequently complicated with scoliosis or uneven shoulder height
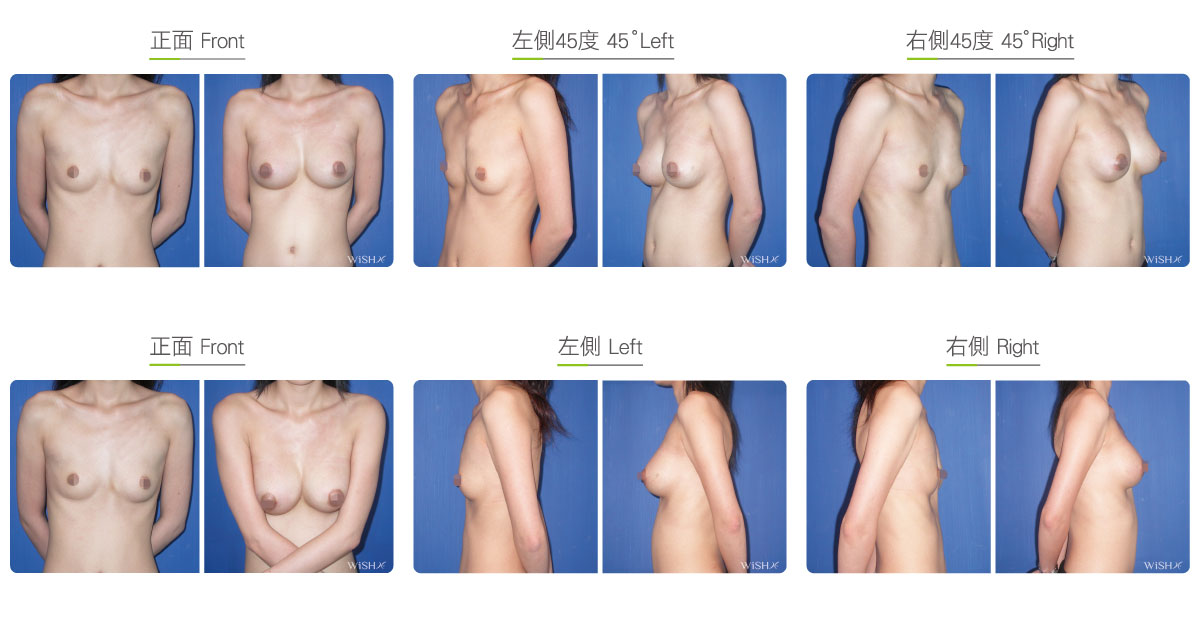
Mild chest asymmetry may not necessitate corrective surgery. However, if one has breasts with more than half a cup difference, which is visibly noticeable, or has combined height differences between the nipples and breasts of more than 1 cm, then breast augmentation should be conducted to correct the problem. This surgery is more complex and time consuming. Here are some special considerations in the technique for this surgery:
- The distance between the two breast pockets needs to be flexibly revised during surgery to realign the breast midline with the body axis.
- A simulating dilator should be used for repetitive measurement and confirmation. Then, implants of different types and sizes or even brands should be adopted and placed.
- The choice of implant may also influence the effectiveness of adjustment. Silicone implants have a fixed volume, and the flexibility and convenience of adjustment are possibly limited; on the other hand, a saline implant filling can be adjusted anytime and is easier to reset breast sizes.
- In severe cases of asymmetry, patients may even need to undergo autologous fat transfer (hybrid mammoplasty) to supplement insufficient implant volume.
- Nipple position and level are difficult to change even when performing breast augmentation in such cases.
Surgical conditions
Duration
- Type of anesthesia: General anesthesia
- Type of incision: Transaxillary, periareolar, or inframammary incision
- Recovery: Within 3 days
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery
- Frequent stretching should be performed for 1 month postoperatively to prevent axillary scar adhesion.
- Tasks and exercises that require excessive arm strength should be avoided, and underwired or push-up bras should not be worn for 3 months postoperatively.
- Smoking and consumption of collagen or vitamin C should be avoided for 3 months postoperatively to prevent the formation of capsules.
- Consistent and regular breast massage should be performed for 6 months postoperatively to maintain breast shape and softness.
Possible complications
- Capsular contracture
- Breasts not completely symmetric
- Breasts/nipples uneven in height
- Scar adhesion (underarms)
- Insensitive or oversensitive nipples (temporary)
- Implant leakage or rupture
Surgical advantages
-
Implants are placed to correct congenital breast asymmetry or skeletal height differences, thus restoring a more even appearance.
-
The procedure can help overcome problems due to breast asymmetry such as limited clothing choices.
-
The results are stable and sustainable.
Surgical drawbacks
-
Implants alone may not achieve completely symmetric breasts.
-
Congenital differences in nipple height cannot be corrected.
-
Although the breasts may appear symmetric, the difference is still palpable.