Dermabrasion
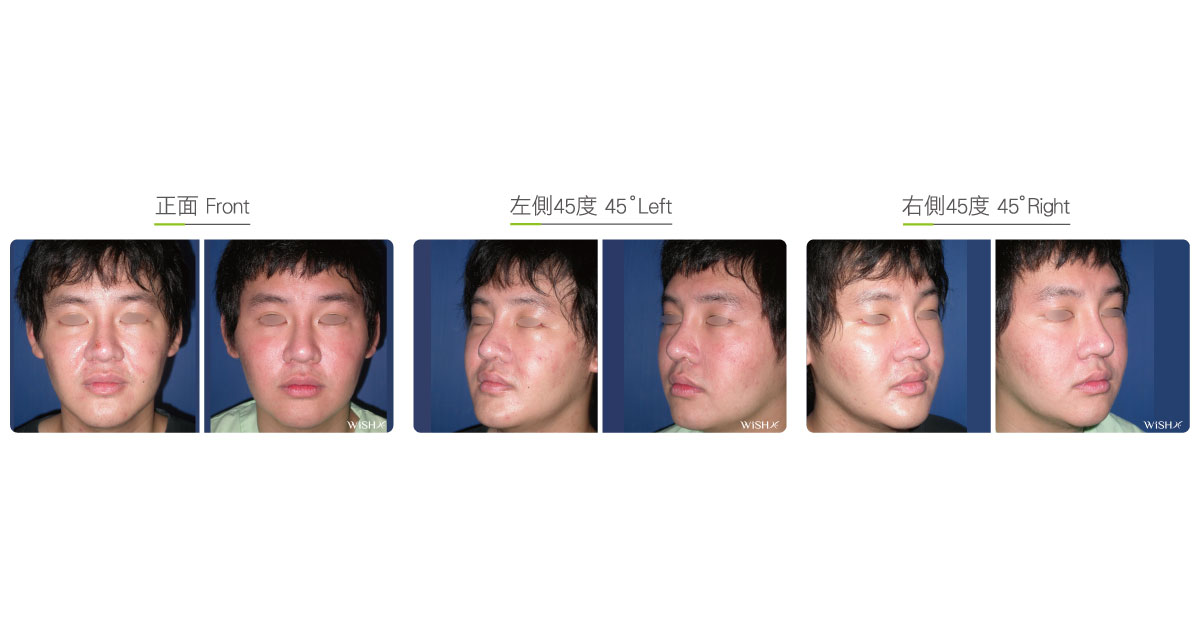
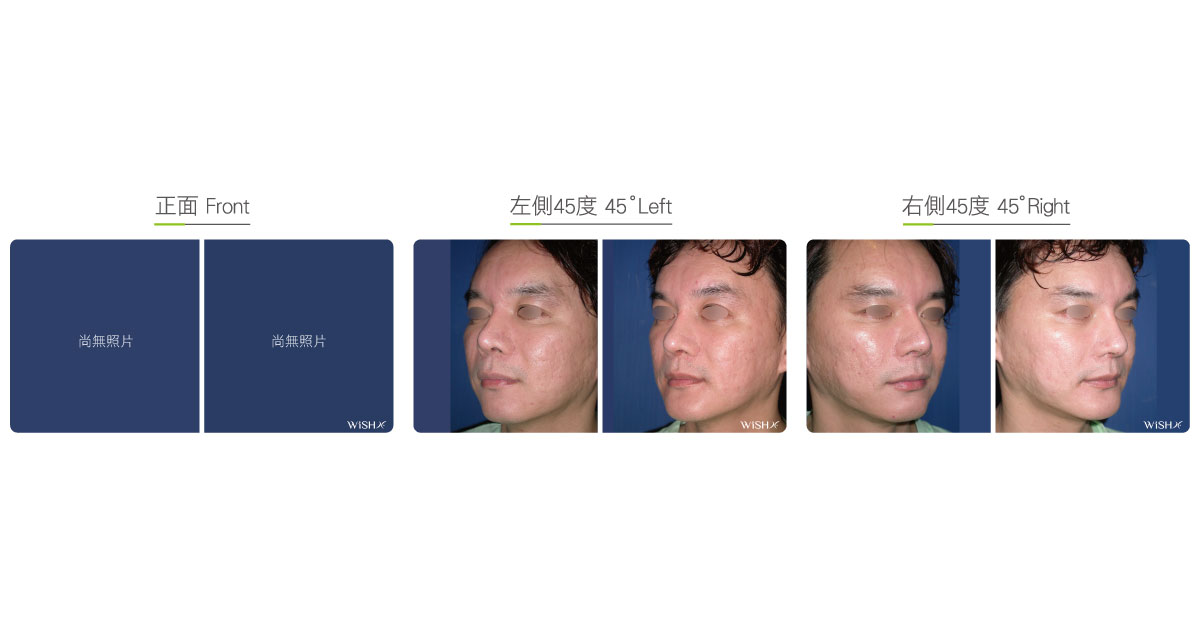
For multiple and large-area acne or smallpox scars, dermabrasion is the only technique for effective and rapid improvement. This technique is based on the mechanical planing of the skin, which enables depressed scars of different depths or sizes to gradually regenerate within a short recovery period and become smooth; therefore, it is also called mechanical dermabrasion. A high-speed diamond burr repeatedly abrades the epidermis and dermis at the whole scar area to level the scar edges and central depression. This process injures the skin and causes it to become red and secrete tissue fluids. In approximately 1 week, dermal cells start to grow and astringe the wound and scar. In the following 1-2 months, the defects of dermabrasion are filled with regenerated skin cells, which ultimately restore the original skin tone and smooth scars. Despite a long recovery period, this technique presents significant results, and each dermabrasion can treat 50% of depressed scars on average. If the patient has severe scar problems, 3 surgeries, at most, are needed to render 70–80% skin smoothness. Therefore, it is still accepted by numerous patients with severe facial depressed spots or orange peel-like skin, and it is also the only feasible treatment method.
The depth of dermabrasion is closely associated with the results and recovery speed, so dermabrasion at different depths is employed based on the severity of the patient’s scar. Superficial dermabrasion is limited at the epidermis and is mainly indicated for patients with sporadic or shallow depressed acne scars and is also used to abrade the stratum corneum to shrink skin pores and make the skin delicate. Its advantage is the rapid astringing of wounds (approximately 3–5 days) and a short recovery period (approximately within 1 month), but the disadvantage is the more courses of dermabrasion. Deep dermabrasion reaches the epidermis and dermis and is used for the treatment of depressed acne scars, smallpox scars, or facial orange peel-like skin. The advantage is the rapid and obvious results and fewer courses of dermabrasion, but the disadvantage is the relatively slow wound healing and a long recovery period (approximately 1–2 months), which is likelier to cause pigmentation and other sequelae. Therefore, patients still need advice from physicians before deciding on a surgical method.
Besides surgical dermabrasion, numerous non-surgical techniques are optional, such as dermabrasion (vaporization) laser, Fraxel, alpha-hydroxy acids, and micro-needle therapy system, for treating depressed acne scars, whose results and cost effectiveness are less obvious than those of dermabrasion. Therefore, if patients accept relatively long recovery periods, mechanical dermabrasion remains the preferred method to treat large-area acne scars.
Comparison Between Surgical Dermabrasion And Laser Dermabrasion
| Dermabrasion surgery | Dermabrasion laser | |
|---|---|---|
| Device used | High-speed electric burr | Carbon dioxide laser, Fraxel laser, etc. |
| Indication | Icicle-shaped acne scars, smallpox scars, and traumatic superficial acne or surgical scars | Rough skin, trauma, or surgical scars |
| Principle of treatment | Mechanical epidermal planing | Thermal stratum corneum shedding |
| Depth of treatment | Epidermis and dermis | Epidermis |
| Method of anesthesia | Fast asleep + local anesthesia | Local anesthesia |
| Skin wound | Temporary skin injury (5 × 7 days) | No |
| Number of courses | Within 3 | 6–10 |
| Treatment interval | At least 3 months | 2-3 weeks |
| Presence of results | Relatively rapid | Relatively slow |
| Risk of darkening | Low | Relatively high |
| Pain | Low | Relatively high |
| Recovery period | Long | Relatively short |
Surgical Conditions
Duration
- Type of anesthesia: Fast asleep + local anesthesia
- Surgical incision: Facial scar
- Recovery: 5–7 days
- Removal of stitches: No
General Instructions
No food and water on the day of surgery
- Frequently change the artificial skin dressing for 1 week postoperatively to prevent wound infection and promote healing.
- Avoid smoking, alcohol, and spicy and irritating foods for 1 month postoperatively to avoid wound healing problems.
- Apply sunscreen for 3 months postoperatively to prevent pigmentation at the site of operation.
- If the wound presents good healing, dermabrasion may be conducted again 3 months after the last surgery.
Ideal Candidates
- Patients with large-area depressed acne and smallpox scars
- Those with sporadic and multiple conical acne scars
- Those with severe uneven facial orange peel-like skin
- Those with depressed linear scars
- Those with coarse facial pores or rough skin
- Those who have received laser dermabrasion but showed insignificant results
Potential Complications
- Pigmentation
- Temporary skin sensitivity or redness
Surgical Advantages
-
It can achieve large-area dermabrasion, whose results are homogenous and natural.
-
There is no need of scar resection, so no scars will be left after the operation.
-
It simultaneously makes the pores and skin delicate.
-
It is less likely to have the risk of darkening associated with laser dermabrasion or rhytidectomy.
-
Results are rapid and obvious compared with those of other surgical methods.
Surgical Drawbacks
-
Surgical extent is large and wound care is complicated.
-
Postoperative recovery period is relatively long.
-
Excess depth of dermabrasion or improper care may result in sequelae such as pigmentation.
-
Postoperative skin may show temporary sensitivity symptoms.