Inverted Nipple Correction
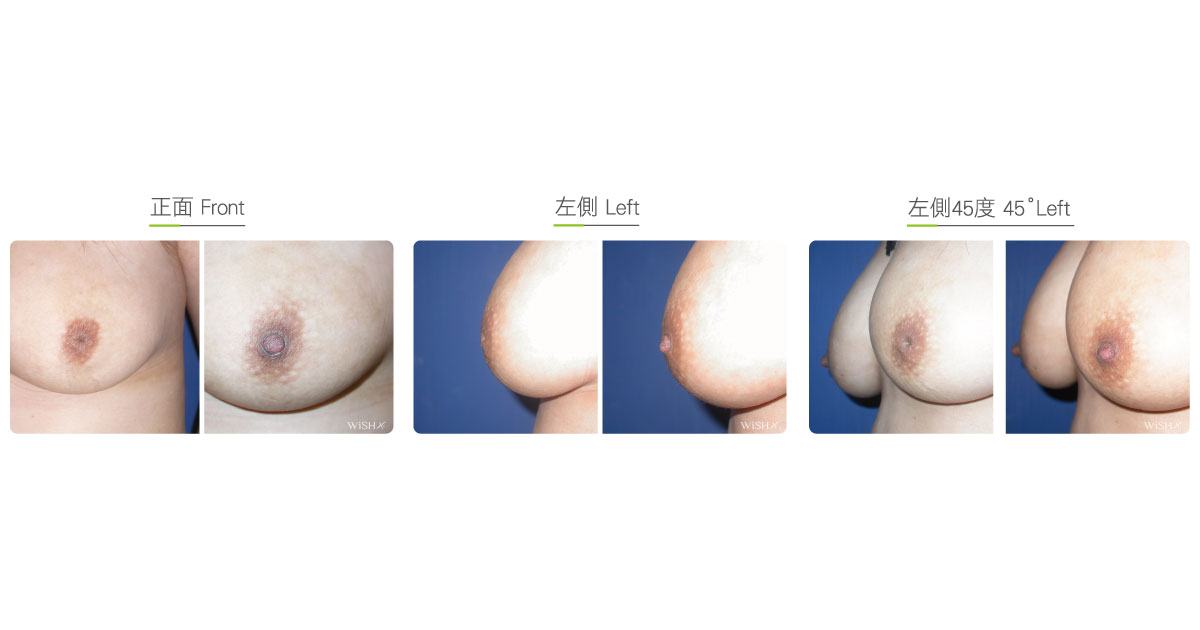
For females, normal nipples should protrude outward, with the whole nipple exposed outside the areola. However, some patients have sinking nipples that look like a volcano or are partially hidden in the areola, which not only affects appearance but also makes cleaning difficult, leading to bacterial growth, odor, secretion, or even inflammation. Moreover, this can make breastfeeding almost impossible or even conceal the early symptoms of malignant breast disease such as nipple discharge. Therefore, patients should seek help from a plastic surgeon to correct sunken nipples.
There are many causes for inverted nipples. The most common cause is congenital dysplasia of the mammary duct and interfascicular connective tissues in the nipples, which induces sinking due to the downward pulling of the mammary duct frenum. This is generally observed in breast development during puberty. Those with mild symptoms can perform a self-directed nipple lifting manipulation for preventive care and observe for any progression. However, if the situation continues to worsen, then corrective surgery can be performed after the age of 20 years is reached. The other cause is side effects related to repeated breastfeeding such as mammary duct atrophy and mastitis. Once breastfeeding ends, patients can undergo corrective surgery as well. Besides the above-mentioned benign causes, patients should pay attention to the sudden inversion of the nipples caused by a few malignant pathologens in the breast. In particular, nipple inversion observed with bloody secretion or strange odor should be diagnosed by breast surgeons first to rule out any malignancy before seeking any nipple adjustment with plastic surgeries.
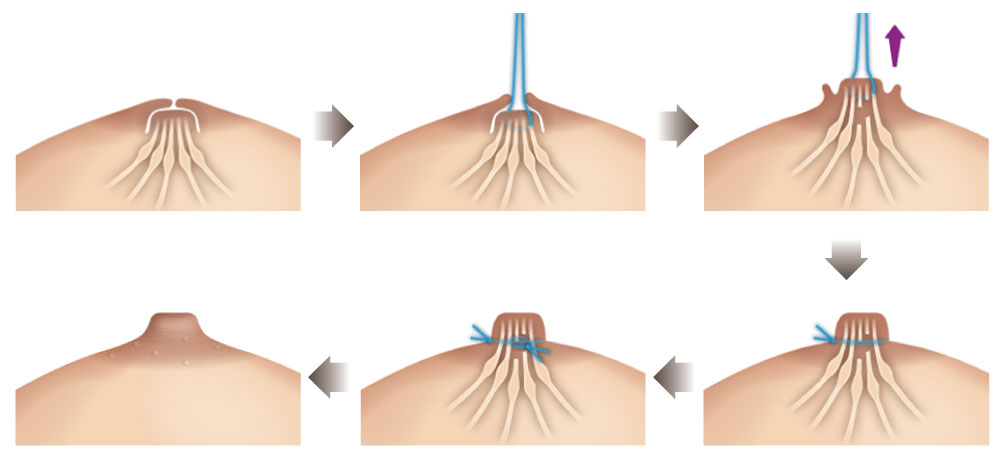
Not all inverted nipples need to be corrected through surgery. In most mild cases, patients can perform a physical stimulation such as self-directed nipple lifting or nipple negative pressure suction, which may present partial prevention and treatment effects. In moderate or severe cases, patients may require corrective surgery to release some tightened lactiferous ducts and frenums to get rid of the downward pull effect. Dr. Chuang performs the newest minimally invasive surgery to correct sunken nipples. Firstly, small incisions (2 mm each) are made on the four sides of the base of the nipple to effectively release the lactiferous ducts and tight ligaments. Secondly, special non-absorbable sutures are planted at the end to stabilize the nipple base. This method has low recurrence, leaves almost no scar, and possibly preserves the ability to breastfeed. It is ideal for many patients, irrespective of whether they are single or married.
Minimally Invasive Inverted Nipple Correction
Inverted Nipple Grading System
| Grade | Symptoms | Treatment |
|---|---|---|
| 1 | A mildly retracted nipple that is on top of the areola; it can be easily pulled out and stay erect thereafter | Frequent nipple lifting |
| 2 | The nipple that is partially or totally submerged into the areola; it can become erect when stimulated; it is not easy to pull out or would quickly retract | Use “nipple braces” or directly correct with surgery |
| 3 | No visible nipple; the nipple is concave like a volcano; it cannot be pulled out with stimulation or force | Inverted nipple correction required |
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Type of incision: 4 small incisions at the nipple base (each approximately 2 mm)
- Recovery: Immediate
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery
- Smoking and alcohol consumption for 3 months postoperatively and the overstimulation of the nipples should be avoided
- Tight clothes that could compress or rub the nipples should not be worn.
Ideal candidates
- Those who lack confidence due to sunken nipples.
- Those with odor or secretion due to the poor hygiene of sunken nipples.
- Those with asymmetrical and unilateral sunken nipples.
- Those with abnormal nipple lumps or bloody nipple secretion.
- Those who are concerned about breastfeeding and on the health of their babies in the future.
Possible complications
- Relapsed sunken nipples (approximately 10% cases)
- Poor nipple circulation
- Nipple atrophy
- Nipple necrosis
- Lactiferous duct obstruction
- Mastitis
- Breastfeeding dysfunction
Surgical advantages
-
Restores normal appearance of nipples and enhances self-confidence.
-
Easier to clean nipples and less likely to deposit dirt.
-
Enhances nipple sensitivity.
-
Avoids overlooking the early symptoms of some malignant pathogens in the breast.
-
Increases intimacy with partner.
Surgical drawbacks
-
The condition may relapse in the future.
-
Occasionally, patients may show nipple oversensitivity.
-
Natural breastfeeding may be impossible (must be assisted by a milking machine).
-
Possible lactiferous duct obstruction or mammary gland inflammation (mastitis).
-
Nipple atrophy or necrosis due to poor circulation.