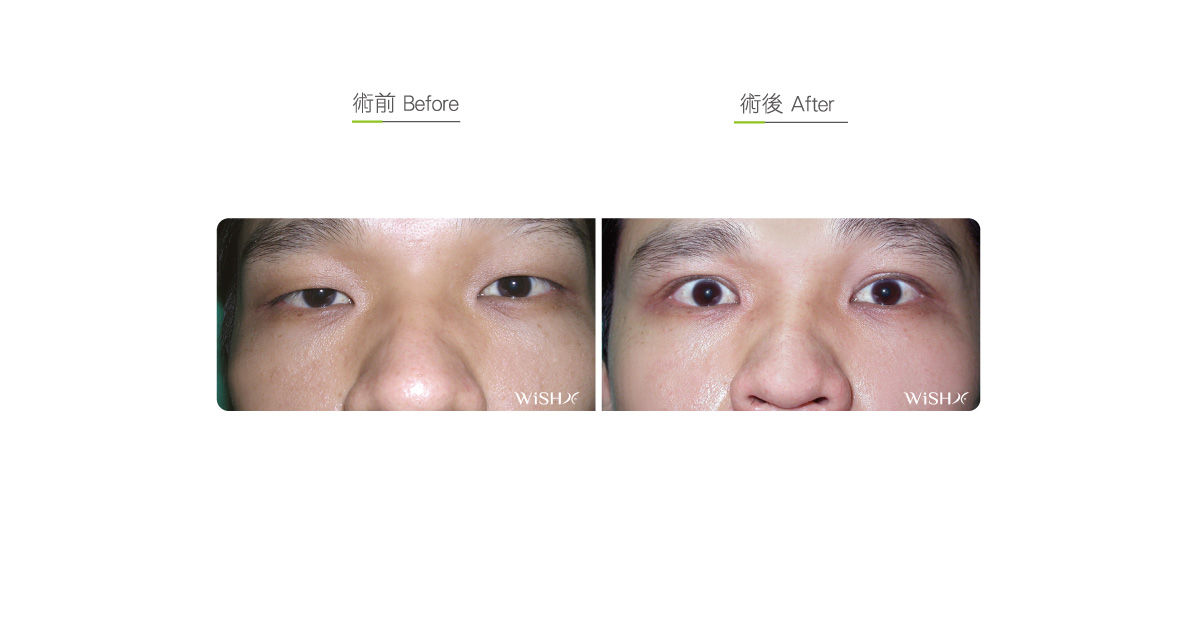
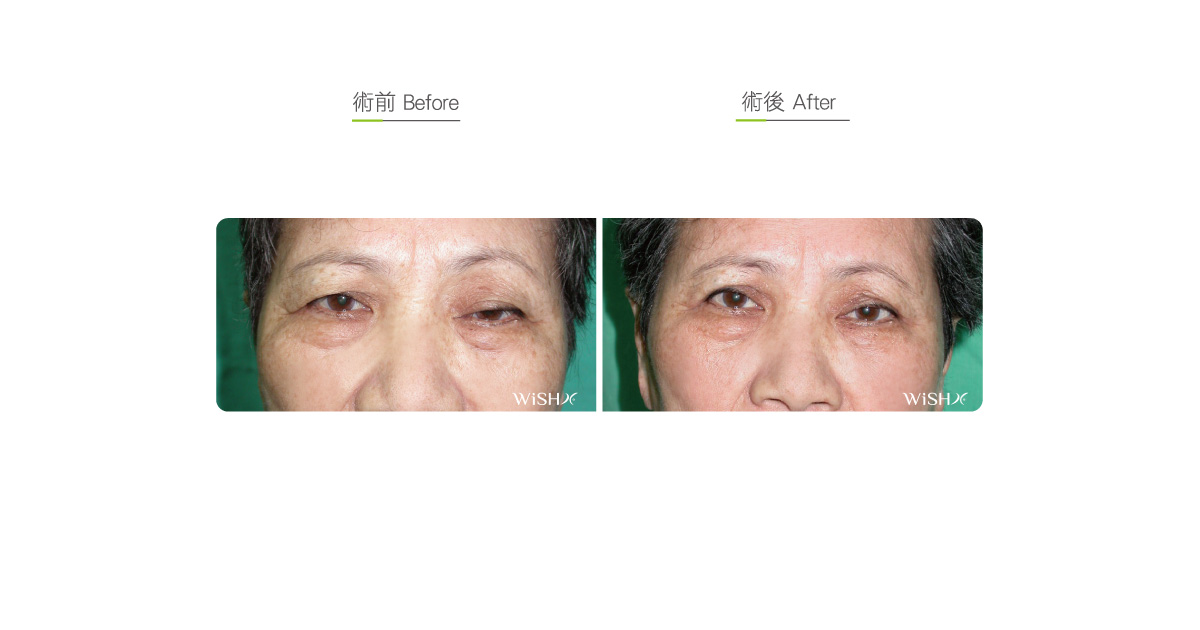
Levator Muscle Correction (Correction of Ptosis)
Levator muscle weakness, also called ptosis, is a common eyelid functional disorder among Orientals, but most symptoms are concealed by monolids or sagged double eyelids. If this underlying problem is not identified during preoperative consultation, it leads to postoperative asymmetry or long-term chronic eyelid edema (blepharedema). Therefore, once the diagnosis is confirmed, levator muscle weakness should be corrected along with double eyelid surgery to avoid probable revision surgery in the future. In addition, some cases of levator muscle weakness (particularly in both eyes) are associated with endocrine diseases, most commonly ptosis caused by myasthenia gravis. Such patients generally normally open the eyes in the morning, but in the afternoon or at night, the eyelids become increasingly heavy or are even hard to raise. In case of similar symptoms, patients may first consult metabolism physicians for diagnosis and treatment, and generally, they only need to take medicines to improve ptosis and do not need to undergo corrective surgery.
From the perspective of the eyelid structure, levator muscles and its aponeurosis are located at the deepest layer of the eyelid and are separated from the eyeballs by only a thin layer of conjunctiva tissue and connect with the eyelash tarsal plate at the distal end. Its primary function is to receive instructions from the brain to contract the muscle and lift the tarsal plate, thus opening the eyes. If congenital defects or prior trauma disrupts or weakens the connection between the levator muscle and tarsal plate, the muscle contracts but the tarsal plate cannot be lifted by the normal force, which is characterized by unequal eyes or a drowsy look like the lazy expression of Garfield. In severe cases the drooping eyelids even cover a majority of the black eyeballs and show no response despite the attempt to open the eyes. Patients always become accustomed to such problems due to the lack of relevant knowledge. However, if left uncorrected in the long term, they gradually affect vision and even become prominent after double eyelid surgery is performed, which results in unequal eyes postoperatively or asymmetrical eyelid folds, thus undermining the surgical results.
Although common people will be unable to determine whether their levator muscle is functioning normally, stringent definitions are stipulated in clinics for treatment reference: in light of the characteristic eyelids among Orientals, when the patient opens the eyelids with a normal force and stares forward, ptosis is graded as follows based on the coverage of black eyeballs by the eyelids:Normal: Superior eyelid lashes cover the upper one-fifth of the black eyeballs
Mild ptosis: Superior eyelid lashes cover the upper one-fourth of the black eyeballs
Moderate ptosis: Superior eyelid lashes cover the upper one-third of the black eyeballs
Severe ptosis: Superior eyelid lashes cover more than the upper one-third of the black eyeballs, or no response when attempting to open eyes
The treatment of ptosis should be based on these criteria of classification. For moderate or severe ptosis, levator muscle corrective surgery should be performed to restore the normal size of the eyes. Mild ptosis is relatively common, and despite its symptoms being within the acceptable range in terms of the monolids among Orientals, many girls who love beauty choose to undergo levator muscle shortening in conjunction with double eyelid surgery, which not only reduces the area of the black eyeballs covered but also completely exposes the eyeballs to sculpt crescent-shaped or big round eyes like dolls; Aesthetically, it is also called eyelid elevation or palpebral fissure enlargement surgery. Moreover, for some patients having already undergone double eyelid surgery, if single eye feebleness or eye asymmetry or even eyelid edema exists for a prolonged postoperative time, consideration should be given to the presence of underlying levator muscle weakness or to the performance of double eyelid repair and levator muscle correction at a proper time.
Levator muscle correction is generally conducted along with double eyelid surgery, and unlike the common double eyelid surgery, it has a relatively deeper surgical field and is more complex. It needs to first dissect the distal fascia of the congenitally defective or lax levator muscle and then fixate the paper-thin aponeurotic tissue to the tarsal plate by a non-absorbable suture, with the fixation position and height adjusted in light of the severity of ptosis. Meanwhile, patients should pay attention to the instructions during the operation to repeatedly open the eyes to allow the physician to achieve accurate positioning; therefore, the surgical time will be extended due to repeated confirmations. After the levator muscle is fixated, the superficial eyelid skins are stitched and fixated to create the double eyelid folds. Regarding the surgical technique, Dr. Chuang currently utilizes partial muscle/aponeurosis resection and stitching that renders the most natural results. During the operation, the distal levator muscle is partially detached from the tarsal plate, and the aponeurosis is then properly resected and shortened before it is stitched to the appropriate position of the tarsal plate. This technique not only avoids ptosis recurrence or eyelid extroversion caused by the traditional muscle plication method but also reduces discomforts that the eyes are unable to be closed and effectively curtails the postoperative swelling to subside and recovery time to rapidly restore natural appearance.
Levator muscle surgery is conducted on a single eye, but it is better to correct both eyes at the same time to ensure symmetry or avoid contralateral compensatory feebleness incurred by single eye correction. This surgery requires a long recovery time, and there should be a waiting period of approximately 3–6 months to confirm the final results. However, despite surgical adjustments, there will be asymmetry or incomplete correction in rare cases. Patients receiving only single eye correction should conquer temporary unequal eyes or uneven double eyelids during the early postoperative period and consider secondary surgery if bilateral eye symmetry cannot be restored after 6 months. Moreover, because there are subjective and objective requirements for levator muscle surgery, patients should fully understand the potential problems of their eyes on consultation before choosing the appropriate surgery.
Dr. Chuang alerts patients who are not suitable for undergoing levator muscle correction under the following circumstances:
- Those with unknown ptosis that may be caused by endocrine disorders (myasthenia gravis)
- Those with exophthalmos or hyperthyroidism
- Those with underlying levator palpebrae muscle excessive exertion or spasm (the superior 1/3one-third white eyeballs are visible when patients hardly open their eyes)
- Those suspected of intracranial nerve compression or disease
- Those being treated for chronic or acute ocular disorders
- Those with glaucoma or high ocular pressure
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: Approximately 1.5–2cm incision at the upper eyelid
- Recovery: 7–10 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Avoid smoking, alcohol, and irritating foods for 1 month postoperatively, and do not wear contact lens.
- Avoid rubbing the eyes and contact with dust and dirty water for 3 months postoperatively.
- Continuously apply warm compresses to the eyelids for 3–6 months postoperatively till the swelling completely subsides.
- In case of a dry eye or eyeball irritation, visit the clinic for examination and treatment.
Ideal candidates
- Patients with moderate and severe congenital ptosis
- Those with acquired ptosis or unequal eyes due to trauma or eye diseases
- Those with mild ptosis but desiring round and big double eyelid surgery (optional surgery)
- Those who underwent have undergone double eyelid surgery that causes iatrogenic or unknown ptosis
- Those having prolong eyelid swelling or thickness not dissipating for over 6 months after double eyelid surgery
Potential complications
- Temporary difficulty in closing the eyes
- Palpebral extroversion
- Oover-correction
- Incomplete correction
- Eyelid asymmetry
- Eyelash defect
- Increased intraocular pressure
- Cornea/conjunctiva scraping or irritation
Surgical advantages
-
It improves palpebral weakness or the problem of unequal eyes problems and restores the normal appearance of the eyelids.
-
It lightens the compression to the eyelids and helps improve vision and ocular fatigue.
-
It alleviates forehead compensatory exertion and mitigates forehead skin laxity and forehead lineswrinkles.
-
Applied for esthetic purposes, it maximizes the eyes in conjunction with double eyelid surgeries (palpebral fissure enlargement surgery).
-
It helps sculpt profound and distinct double eyelids.
-
It modifies partial eyelash inversion problems.
Surgical drawbacks
-
It is difficult to position the fixation site of the levator palpebrae muscle, which may result in excessive or incomplete correction. In case of distinct asymmetry, secondary surgery should be conducted.
-
It may incur temporary difficulty in closing the eyes or chronic conjunctival irritation and other discomforts.
-
It may result in temporary blurry vision or diplopia.
-
It may lead to temporary palpebral extroversion or asymmetry.
-
It may cause eyeball dryness or aggravate other chronic problems.