Philtrum Reduction
The philtrum is located between the nose and upper lip, from the bottom of the columella to the upper margin of the procheilon, and its length varies along with individual face shape (1.8–2 cm on average). With the physiological functions of connecting the nose and upper lip, an exceedingly long philtrum is prone to expose the defects of upper palate prominence or upper lip droopiness and is unable to expose teeth or tooth crevices on smiling, which makes people appear serious or senile. A long philtrum even affects the proportion of the midface and results in an exceedingly long midface, so philtrum reduction is considered. The causes of a long philtrum are numerous, such as congenital upper palate prominence (mouth protrusion), excess development of midface skeleton, retracted or too short columella, or philtrum skin laxity due to orthognathic surgery. Nevertheless, not all long philtrums can be redressed by philtrum reduction, and patients should confirm with the physician about the cause and feasibility of improvement before the operation.
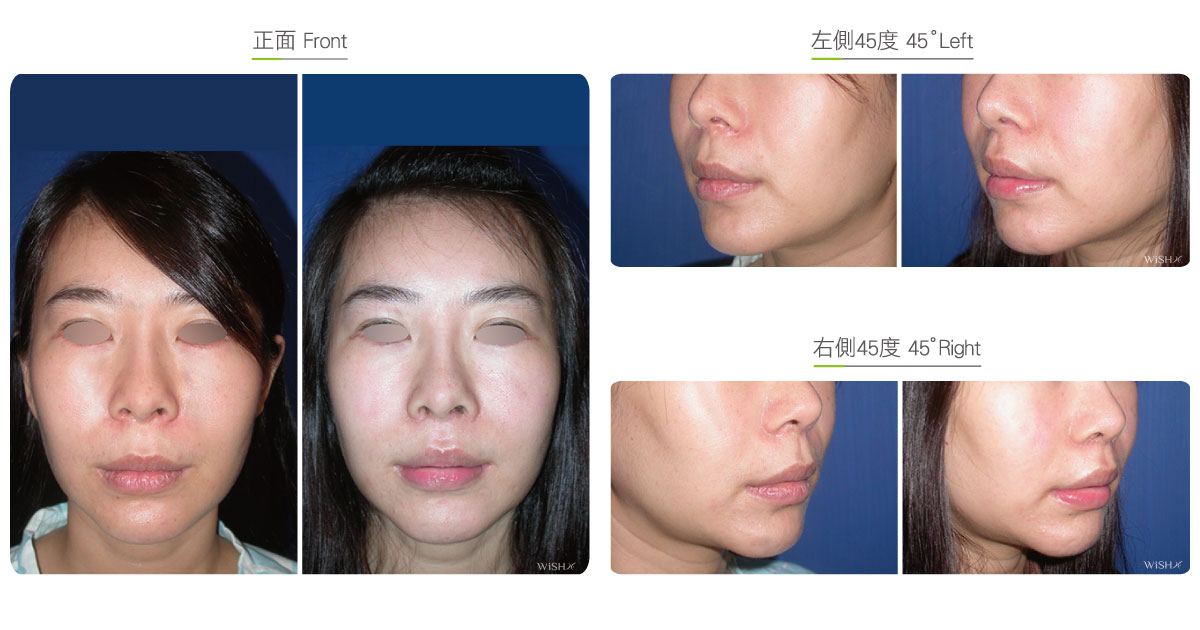
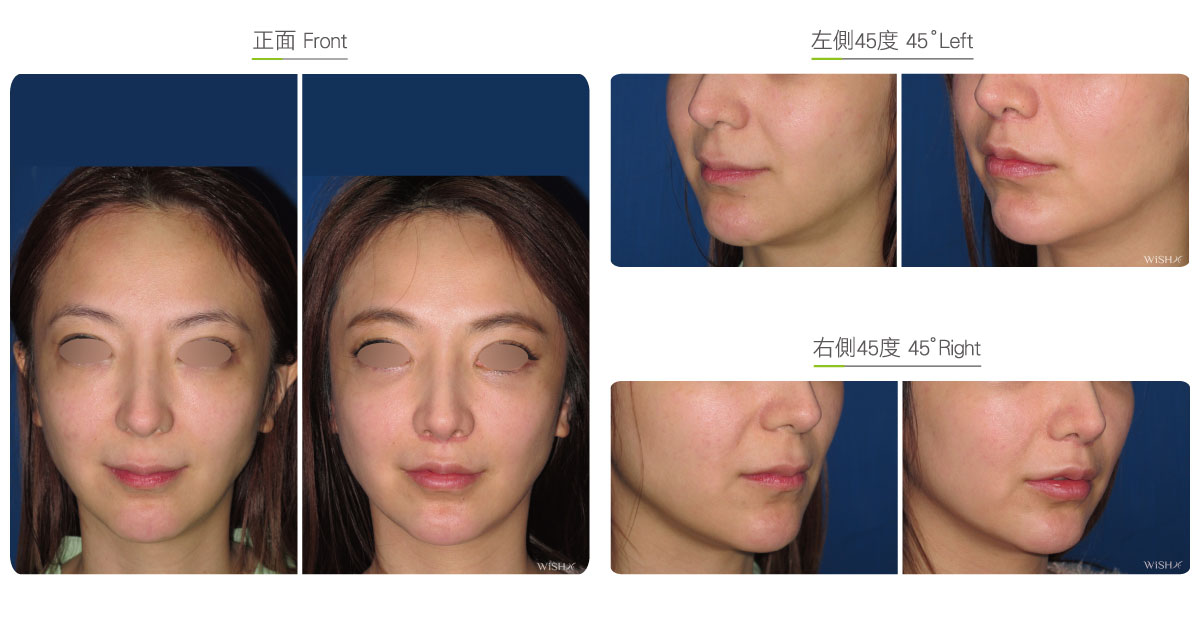
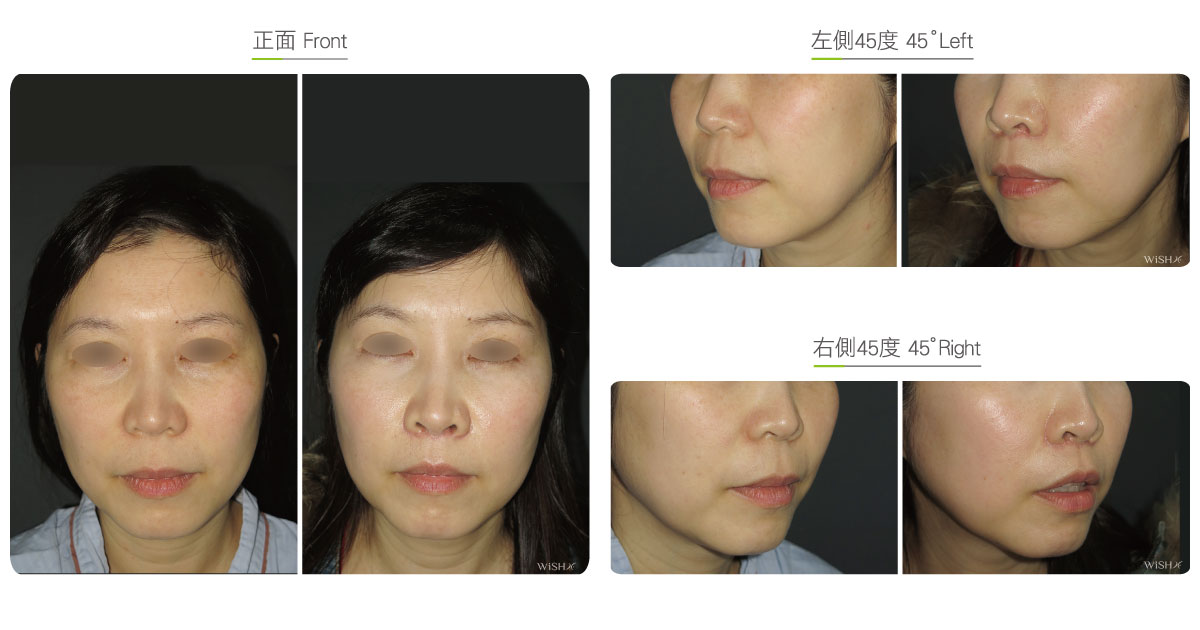
Simple philtrum reduction is also called upper lip lift as the surgery not only shortens the philtrum but also elevates the upper lip angle to sculpt a youthful appearance of a mildly projected lip. An incision is made at the connection between the alar margin and the columellar bottom, with proper skin excised (usually about 0.5-0.8cm), and then, the distal skin of the resection close to the upper lip is advanced upward and stitched to the ala nasi and columellar base. Thus, the upper lip, including the mouth corner, can be lifted upward, which not only effectively shortens the philtrum but also sculpts the projected lip and maximally conceals the scar at the bottom of the nose. Nevertheless, the surgical incision is relatively long and induces scarring afterword, and both ends of the stitches can be stretched by tension from speaking or squeezing, which affects the columellar angle, or even cause nostril exposure or alar deformation in overdone cases. Therefore, the nose shape of the patient should also be factored in during preoperative evaluation. Patients with a congenital snub nose or nostril exposure are recommended to first undergo rhinoplasty or alar reduction before philtrum reduction, which conceals the scar at the shadow of the nasal base.
Modifications of Endonasal lip lift :

Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Type of incision: At the connection between the bilateral alar margins and the columellar bottom
- Recovery: 3–5 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Avoid smoking, alcohol, and irritating foods for 1 month postoperatively, and avoid laughing or singing or other overt mouth opening behaviors.
- Take care of the scar for 3 months postoperatively to avoid scar hyperplasia.
Ideal candidates
- Patients whose philtrum is longer than 2 cm
- Those with upper lip droopiness due to an exceedingly long philtrum
- Those with philtrum and upper lip skin laxity due to a prior orthognathic surgery
- Those with a long philtrum due to upper palate prominence (mouth protrusion or osseous snaggletooth)
- Those with upper lip laxity due to dental and palatine correction by orthodontics
- Those who hope to shorten their midface proportion
Possible complications
- Scar hyperplasia
- Nostril exposure
- Alar stretching
- Tooth exposure
- Difficulty in closing the mouth
- Skin paresthesia
Surgical advantages
-
It effectively reduces the philtrum within the normal scope.
-
It concurrently elevates the upper lip angle to sculpt a projected lip.
-
It effectively shortens the visual proportion of the midface without performing a major orthognathic surgery.
-
It resolves the complication of upper lip skin laxity because of orthognathic bone surgery or orthodontic correction.
Surgical drawbacks
-
The surgical incision is relatively long and may leave a scar.
-
It may change the shape of the columella, ala nasi or nostril.
-
The skin around the upper lip or ala nasi may present numbness or insensitivity.
-
Excess correction may result in tooth exposure or difficulty in closing the mouth.
-
Once the skin is over excised, it is unable to be restored.