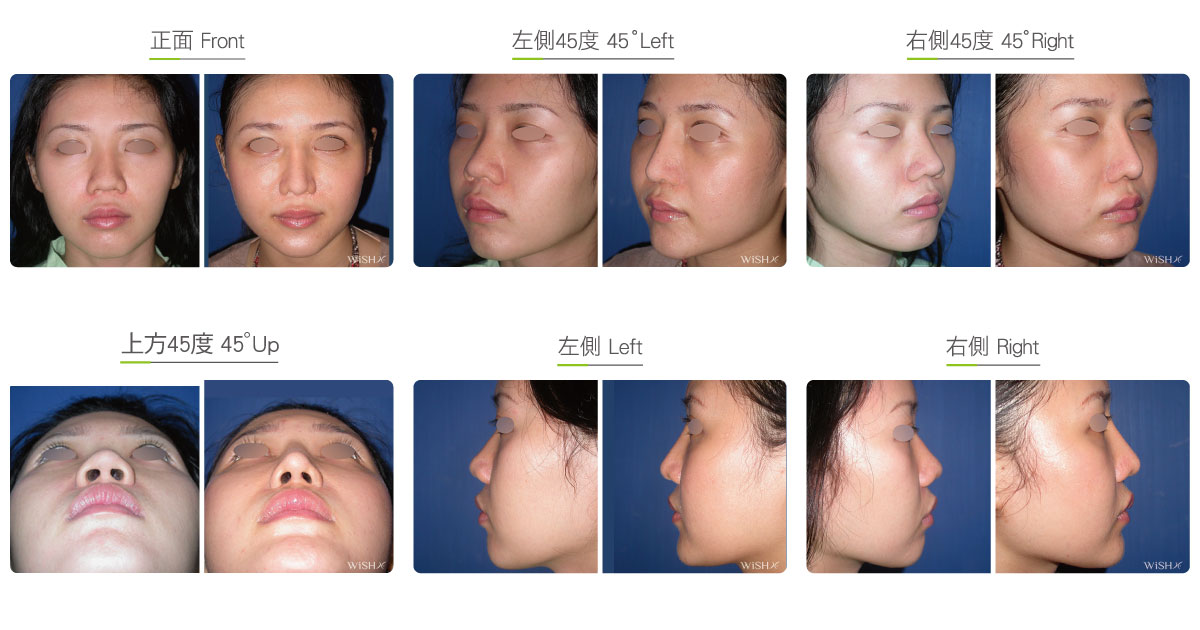
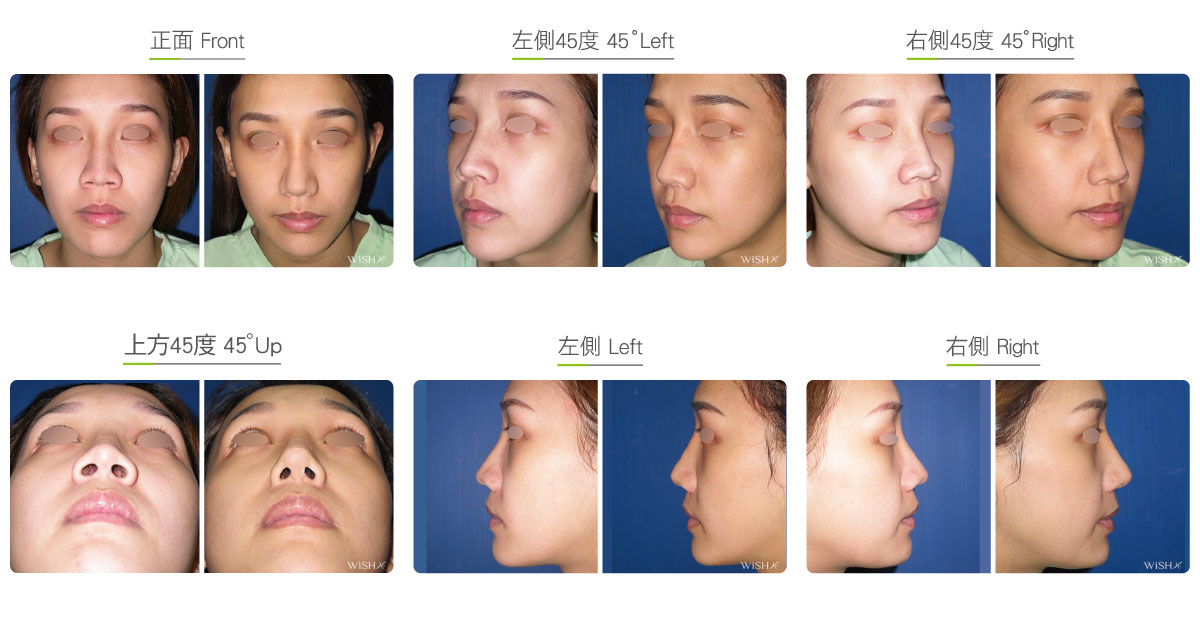
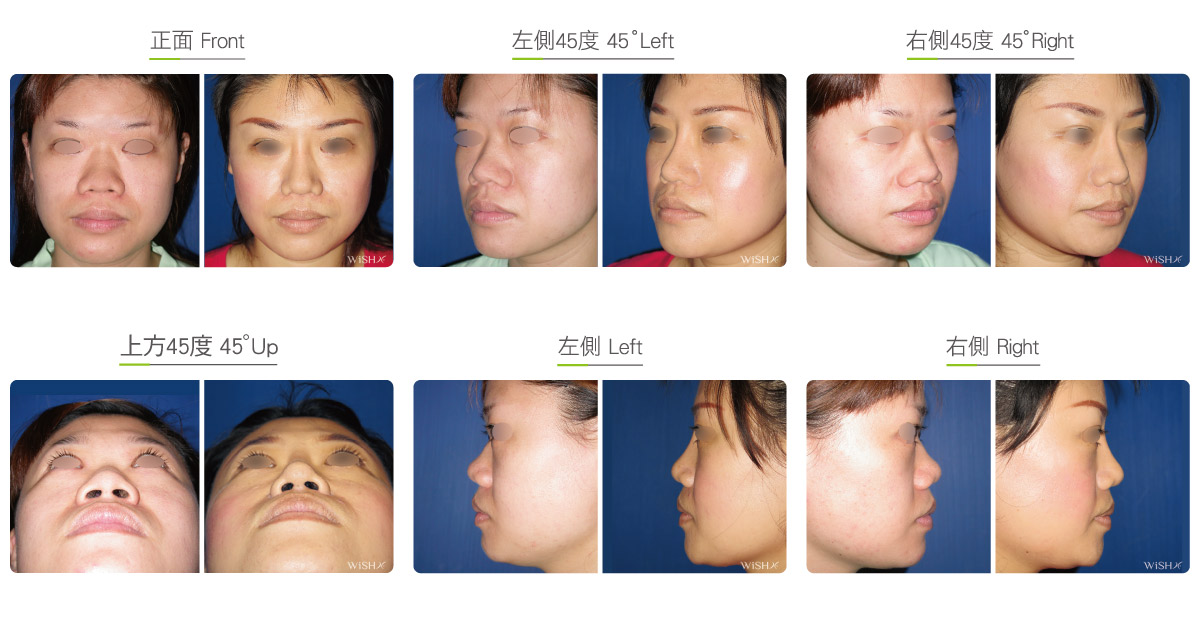
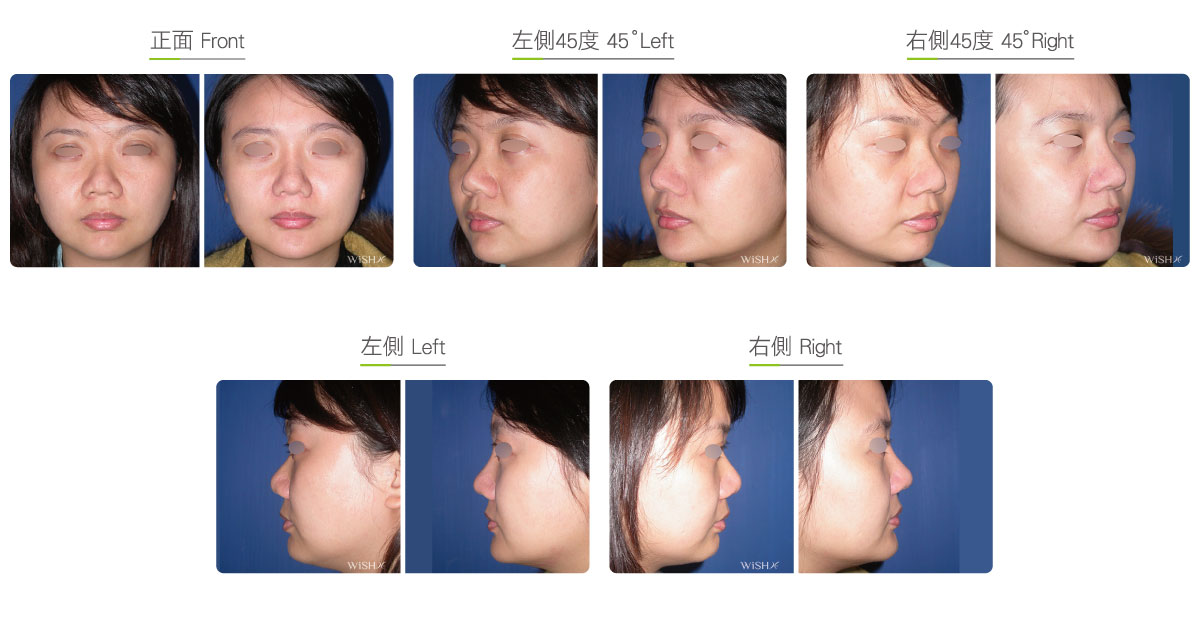
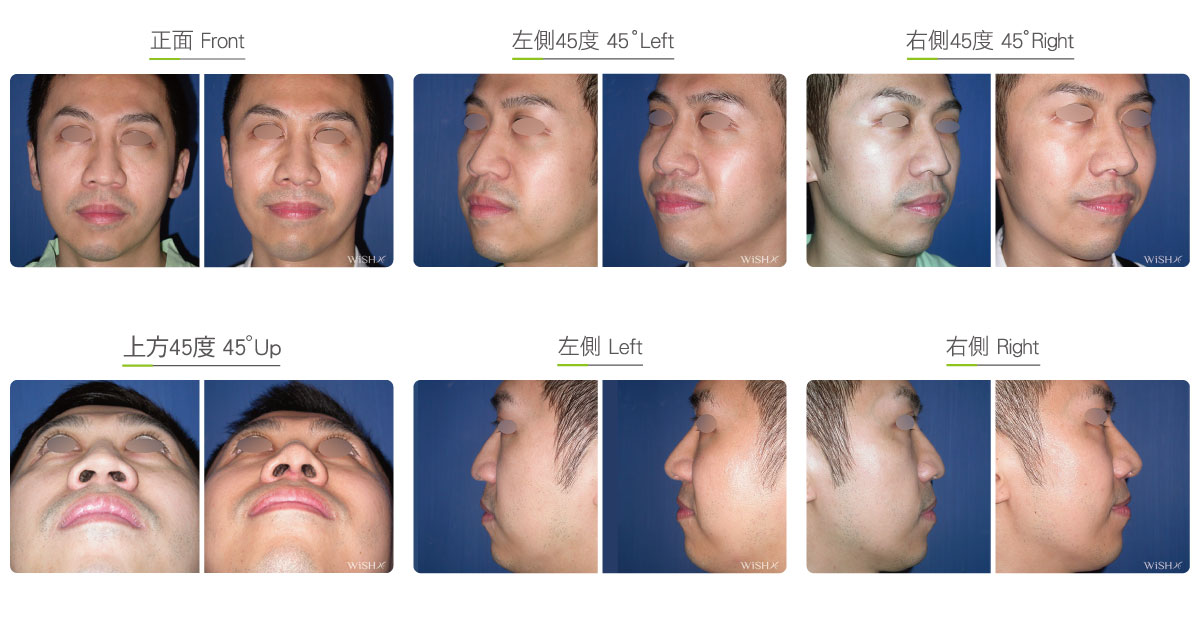
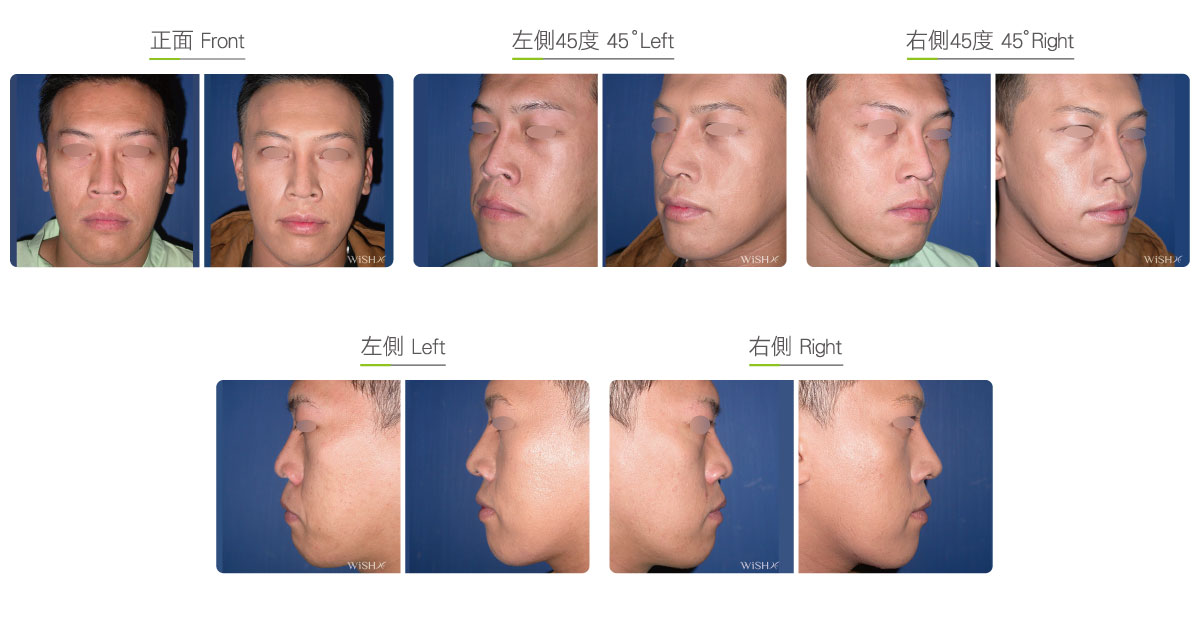
Constricted Nose Correction
This is also called columellar elongation surgery. The nasal columella is located at the middle of the two nostrils and connects the osseous structure of the upper palate at the inferior end, supports the nasal tip structures and lower lateral (alar) cartilages at the superior end, and links with the nasal septal cartilage at the posterior wall. It is a very important structure in nasal tip sculpting. Under normal circumstances, the nasal columella extends to the same height of the bilateral alar feet. If the columella retracts to above the horizontal line of the alar feet from the frontal view or the nasal columella intersects with the upper palate by an angle greater than 90° or is even concealed by the nasal tip, it amounts to obvious columellar retraction and should be corrected by columella elongation surgery. In this surgery, it is necessary to make an incision at the bottom of the columella and harvest the auricular cartilage and partial septal cartilage to be fixated at the front of the nasal septum to extend the columella below the horizontal line of the alar feet, which makes the columella and bilateral nostril upper margins present a curvature similar to that of a sea gull wing and reproduce the marble-shaped supra-tip with the nasal tip extending downward. This surgery is generally combined with open (Korean-style) rhinoplasty or separately conducted for nasal tip sculpting (open tiplasty).
Because the skin adjacent to the columella is mostly very tight and insufficient in most cases, abundant cartilages or even skin grafts may be harvested to render good results. If sufficient cartilage is not harvested due to congenital aplasia of the nasal septum, some patients with severe columellar retraction should consider autologous or homologous costal cartilage transplantation for better improvement. If there is short of skin for coverage, patients may need to harvest composite auricular grafts to secure the wound healing.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: At the bottom of the nasal columella and inside the bilateral nostrils
- Recovery: 5–7 days
- Removal of stitches: 7 days
General instructions
Fast from food and water on the day of operation
- Avoid smoking and alcohol and impacts or compressions to the nasal tip for 3 months postoperatively, and clean the intranasal wound in the morning and evening every day.
- Abstain from eating raw food, seafood, and irritating food or spices for 3 months postoperatively.
- Avoid exposure of the nostrils to dirty water (sea water, swimming pool or sauna water, and hot springs) and close contact with pets and dust mites for 3 months postoperatively.
Ideal candidates
- Patients with nasal columella retracting above the horizontal line of the nasal tip or alar feet
- Those with an obvious congenital hook nose
- Those who have undergone open (Korean-style) rhinoplasty but still feel that its nasal columella is too short
- Those with nasal columellar contracture due to the prior infection or removal of a nasal implant
Potential complications
- Scarring
- Exceedingly long nasal tip
- Incomplete correction
- Poor wound healing
Surgical advantages
-
It is able to solve columellar retraction and restore the normal nose shape.
-
It is able to sculpt a charming angle and curvature of the marble-shaped nasal tip.
-
The surgical results are stable and persistent.
Surgical drawbacks
-
It may cause partial exposure of the nostrils.
-
Excess elongation of nasal columella is prone to result in a long nose shape.
-
Partial cartilage may be absorbed, which may compromise the results.