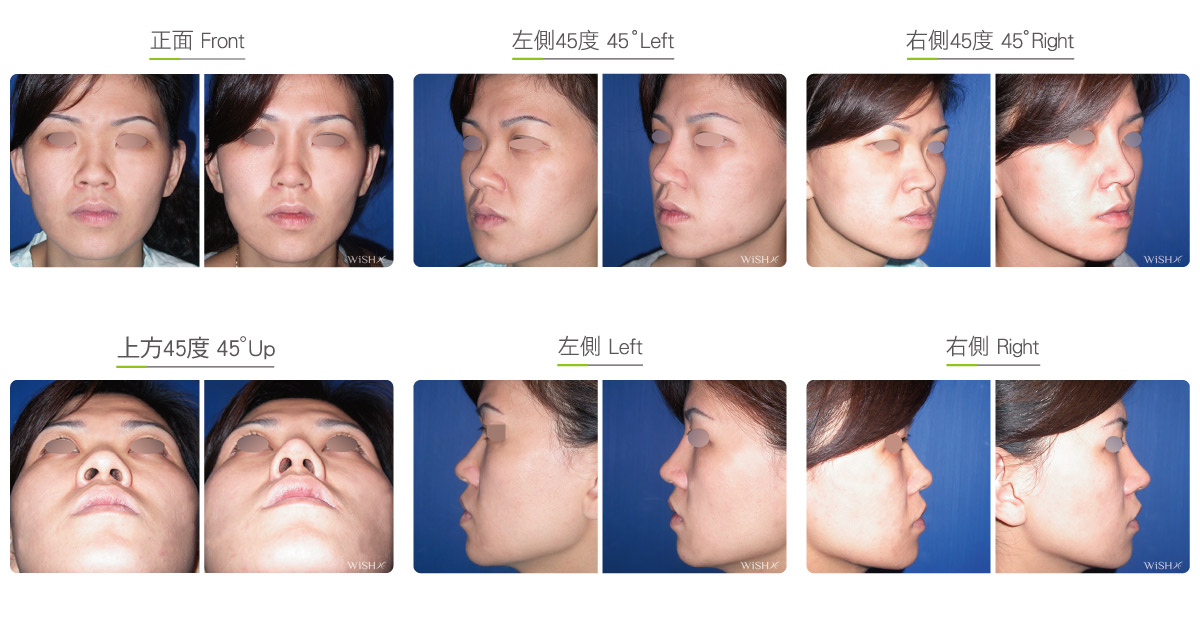
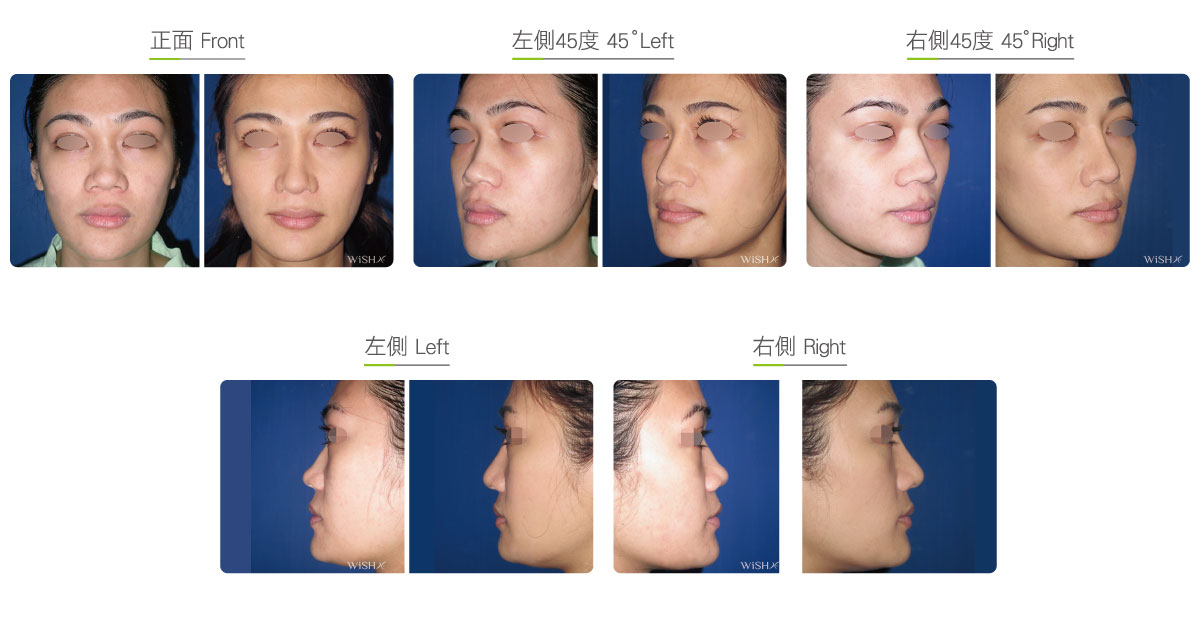
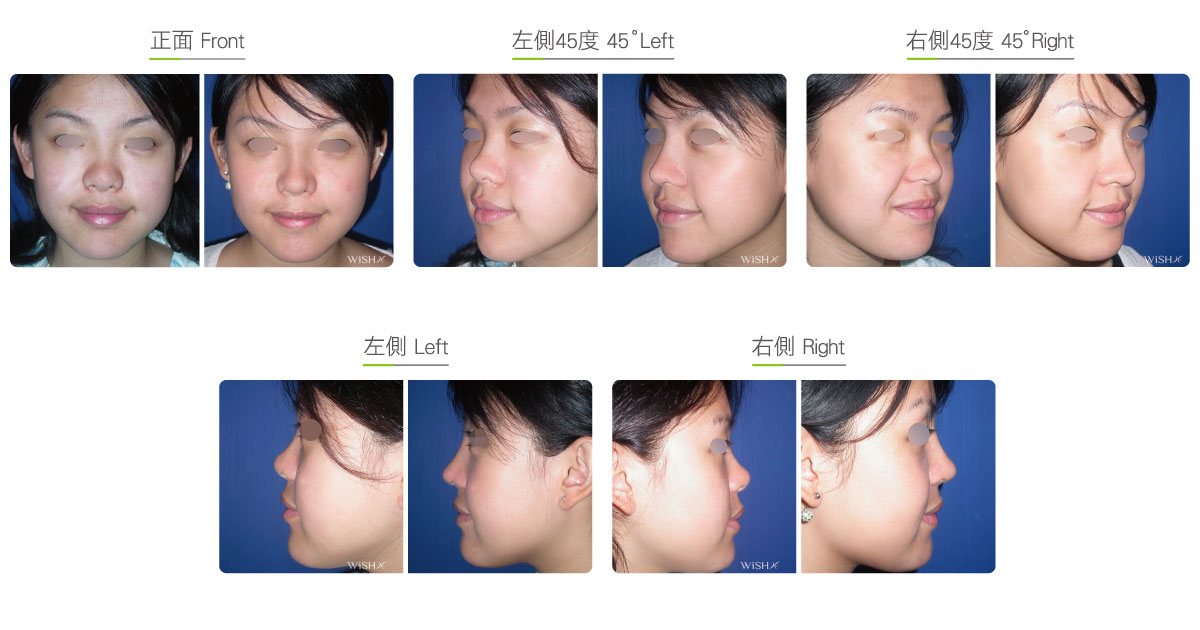
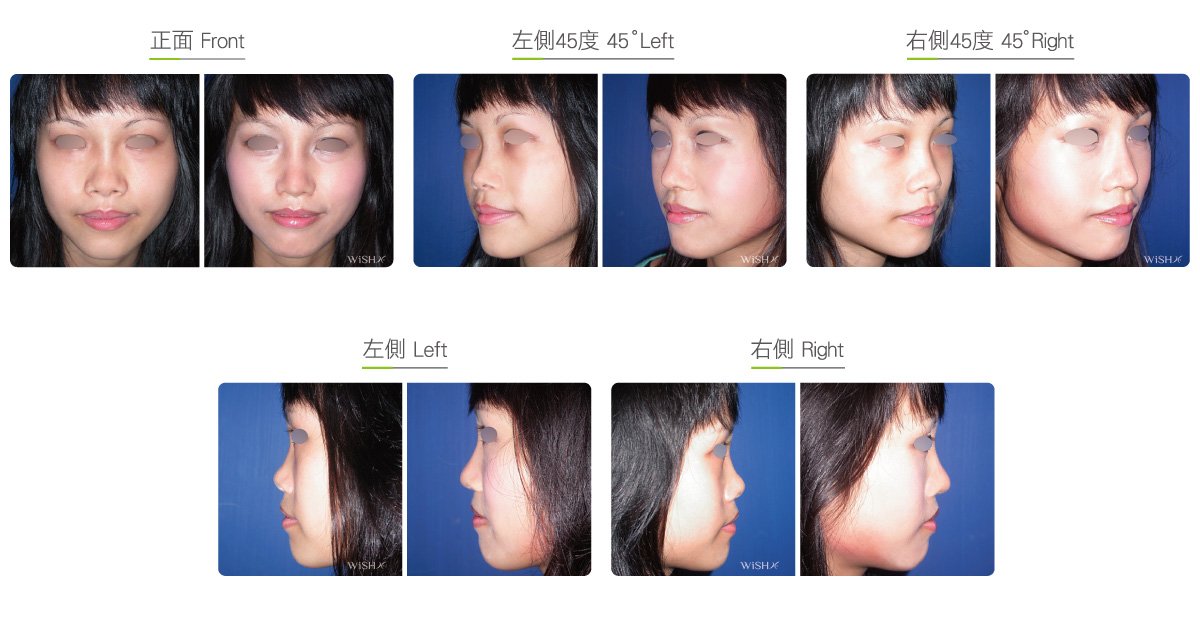
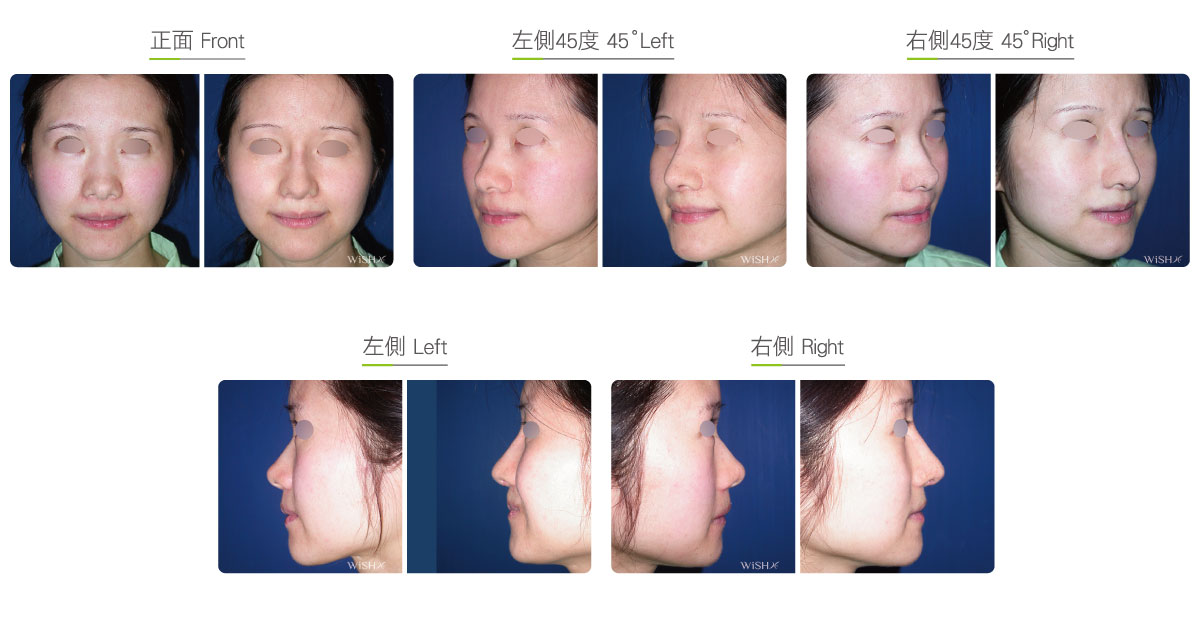
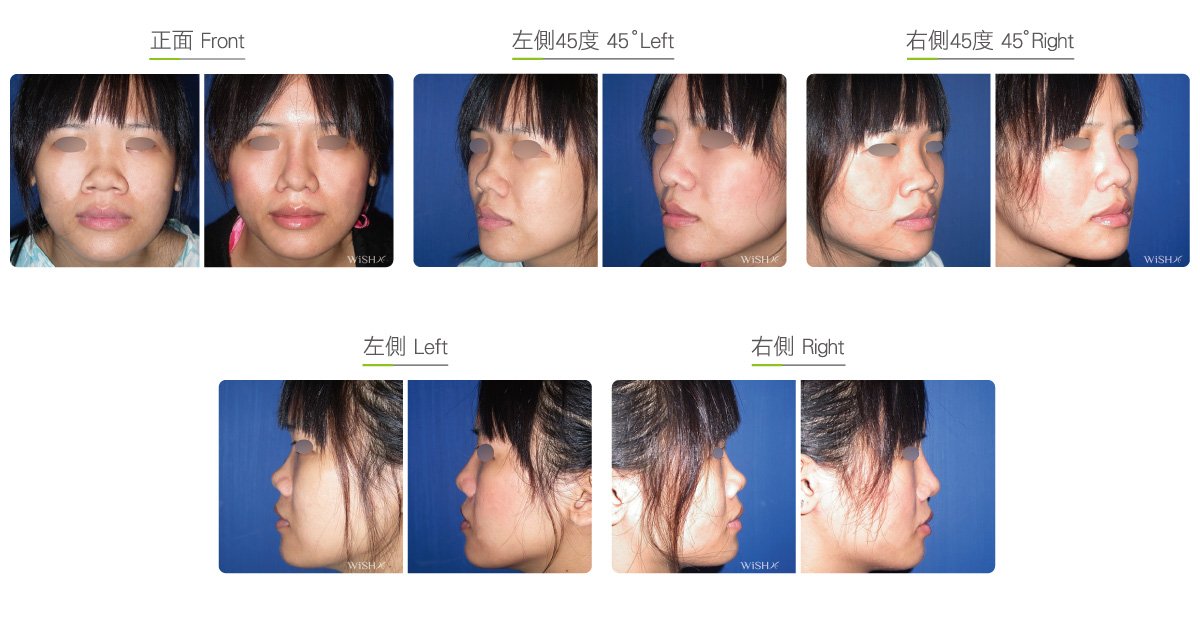
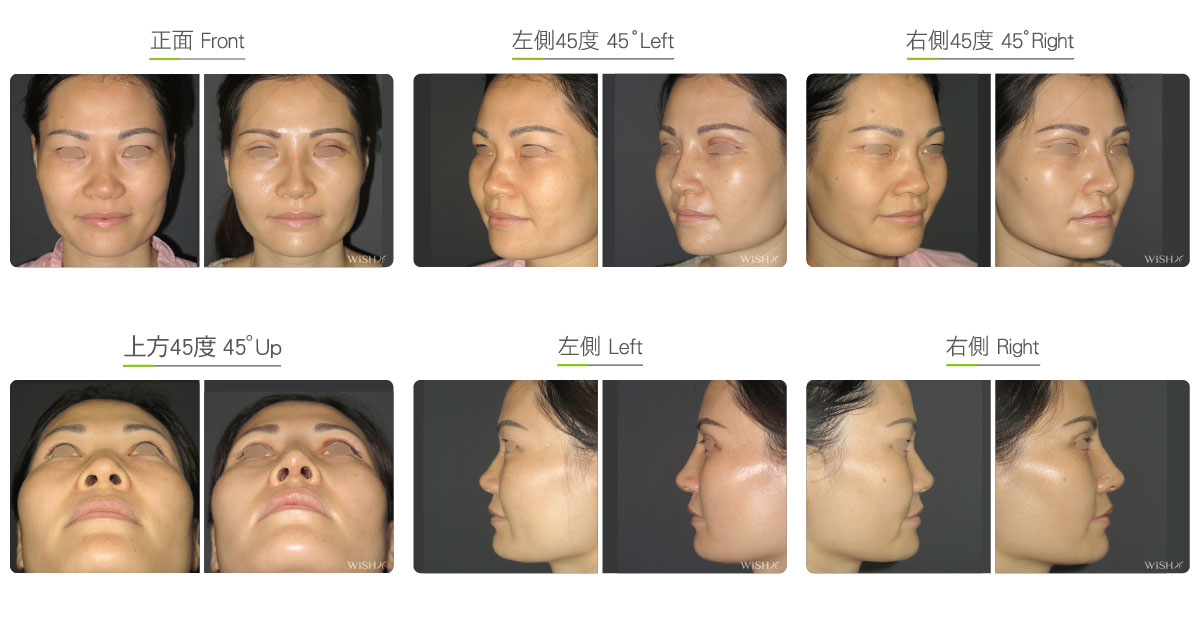
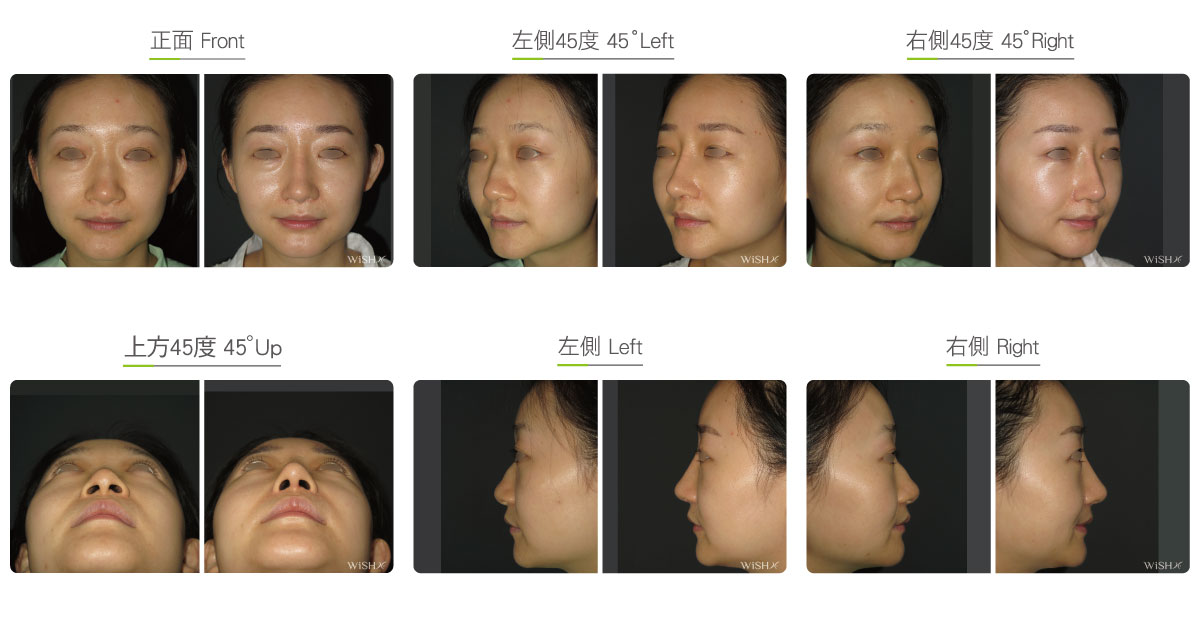
Saddle Nose Correction
Saddle nose mainly manifests as an irregular concavity in the middle of the nasal bridge from the lateral view, similar to the U shape of a saddle, or no continuous linkage between the nasal bridge and nasal tip from the frontal view, presenting an S-shaped deviation. This problem is not rare among patients undergoing rhinoplasty, particularly in females. It is generally associated with the congenitally poor connection between the nasal septum and nasal bridge bone, and in some cases, it is attributable to the detachment of the nasal bridge from the nasal septal cartilage because of traumatic impacts. Because many patients with saddle nose have concurrent nasal septal deviation and nasal obstruction or a congenitally relatively low radix or even an upturned nose, Korean-style (open) rhinoplasty or lateral osteotomy will be simultaneously performed for comprehensive correction. Surgeries on this nose type need to use nasal implants (silicone or Sili-Tex prosthesis) to improve the height of the nasal bridge and compensate the depression at the middle nasal bridge and also require additional autologous auricular cartilages to sculpt the nasal tip and reinforce the columella because the congenital septal cartilage usually has warping or inadequate hardness. Additionally, Dr. Chuang evaluates whether the support of the middle section of the nasal bridge is sufficient; otherwise, extra flaky Gore-Tex materials need to be emplaced above the nasal septum to strut the nasal implants, namely, the composite rhinoplasty, to ensure the stability and form of the nasal bridge in the long term.
Surgical conditions
duration
- Type of anesthesia: IV sedation + local anesthesia or general anesthesia
- Surgical incision: At the bottom of the nasal columella and inside the bilateral nostrils
- Recovery: 5–7 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Wear a tape or nasal plaster splint for 1 week postoperatively to stabilize the nasal bridge.
- Avoid smoking and alcohol and impacts or compressions to the nasal tip for 3 months postoperatively, and clean the intranasal wound in the morning and evening every day.
- Abstain from eating raw food, seafood, and irritating food or spices for 3 months postoperatively.
- Avoid exposure of the nostrils to dirty water (sea water, swimming pool or sauna water, and hot springs) and close contact with pets and dust mites for 3 months postoperatively.
Ideal candidates
- Patients with congenital depression at the middle section of the nasal bridge like a saddle
- Those with deviated nasal bones due to fracture at the connection with the nasal septum from external impacts or trauma
- Those with nasal septal deviation or nasal obstruction due to nasal bridge collapse
Potential complications
- Nasal bridge collapse or deviation
- Nasal obstruction or disturbance in respiration
- Incomplete correction
- Nasal implant shift
Surgical advantages
-
It is able to conceal nasal bridge collapse by rhinoplasty and restore the normal appearance of the nose.
-
It is able to simultaneously redress functional disturbances such as nasal septal deviation.
Surgical drawbacks
-
Due to the weak support to the nasal bridge, the stability of the nasal implant may be poor.
-
Cartilages need to be harvested from multiple sites to correct the collapse and defects of the nasal septum.
-
Nasal septal deviation may not be completely corrected.