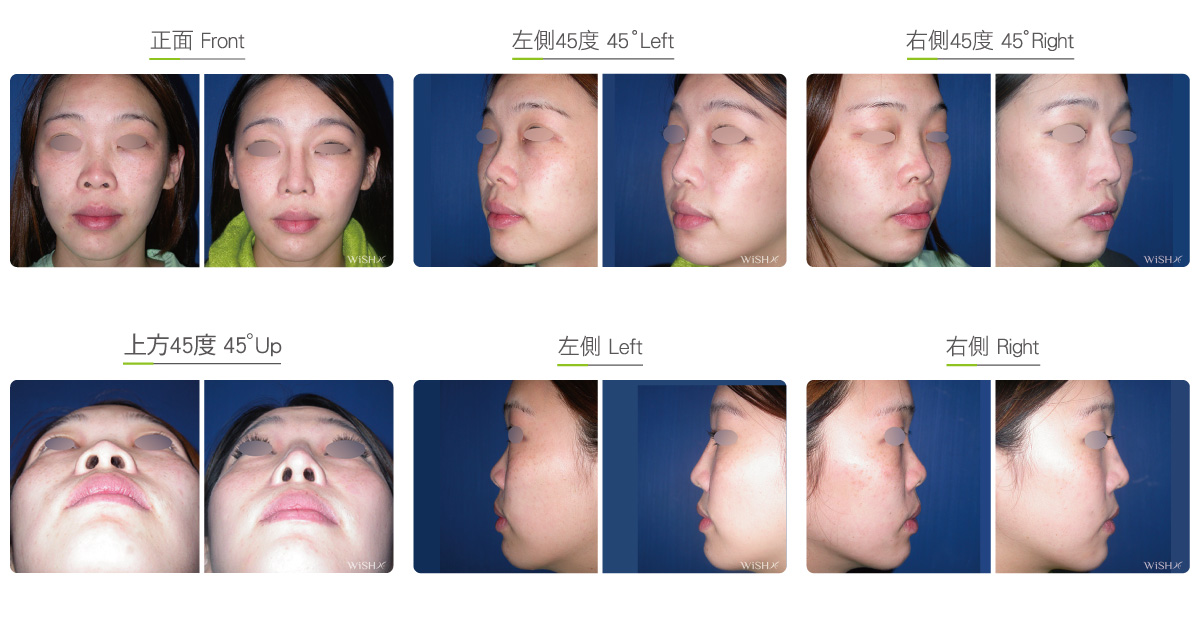
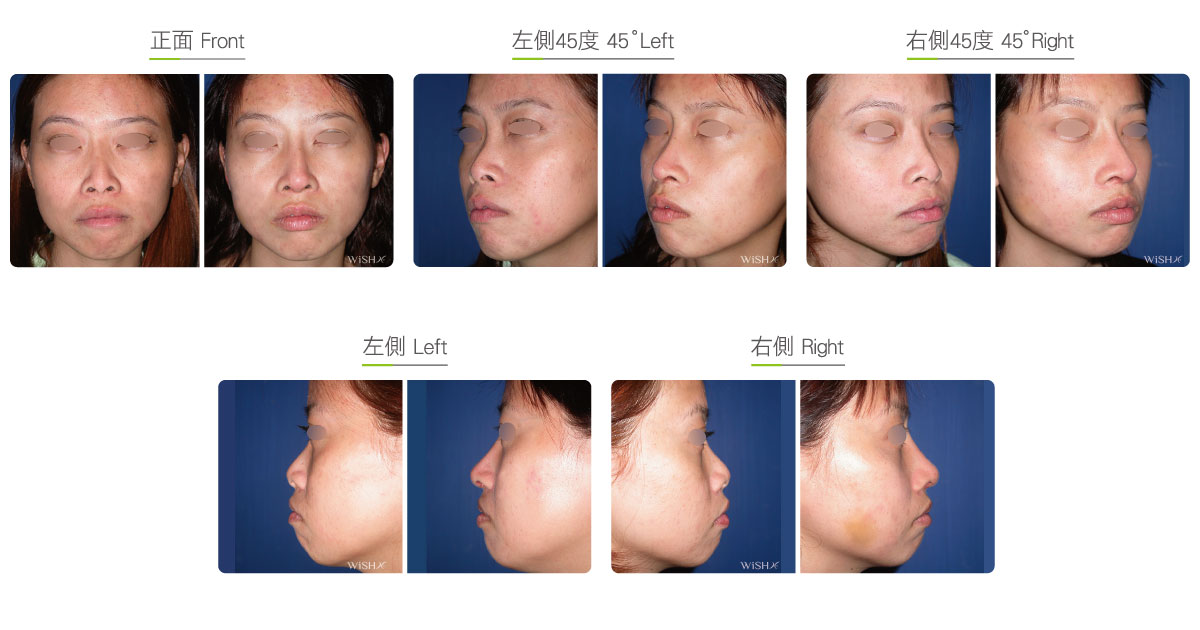
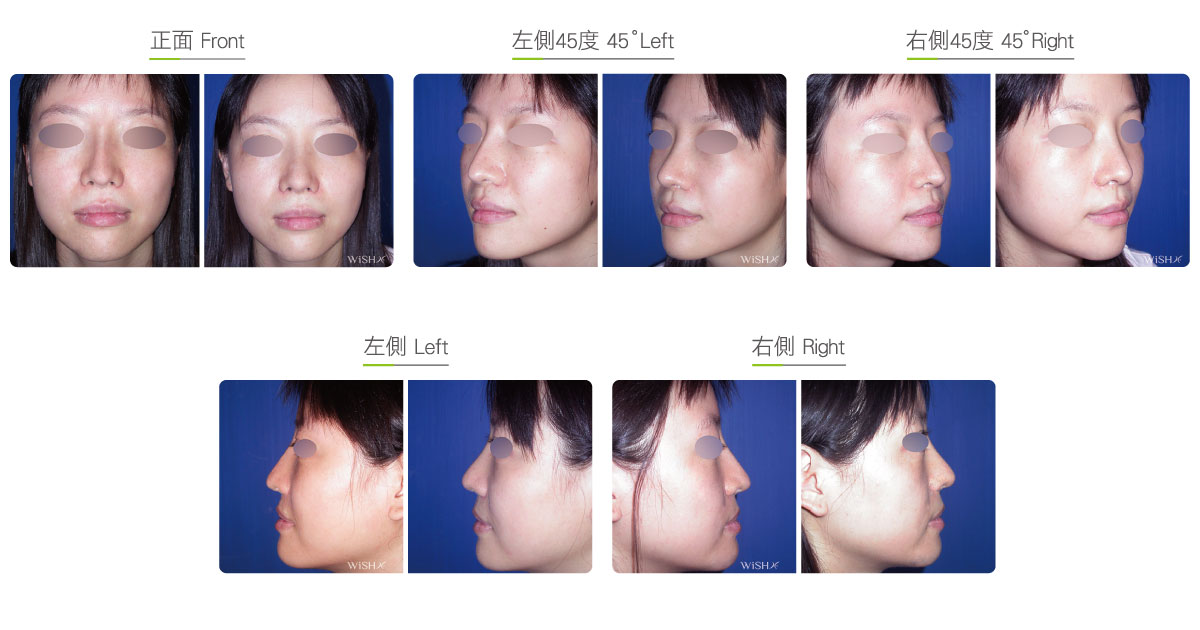
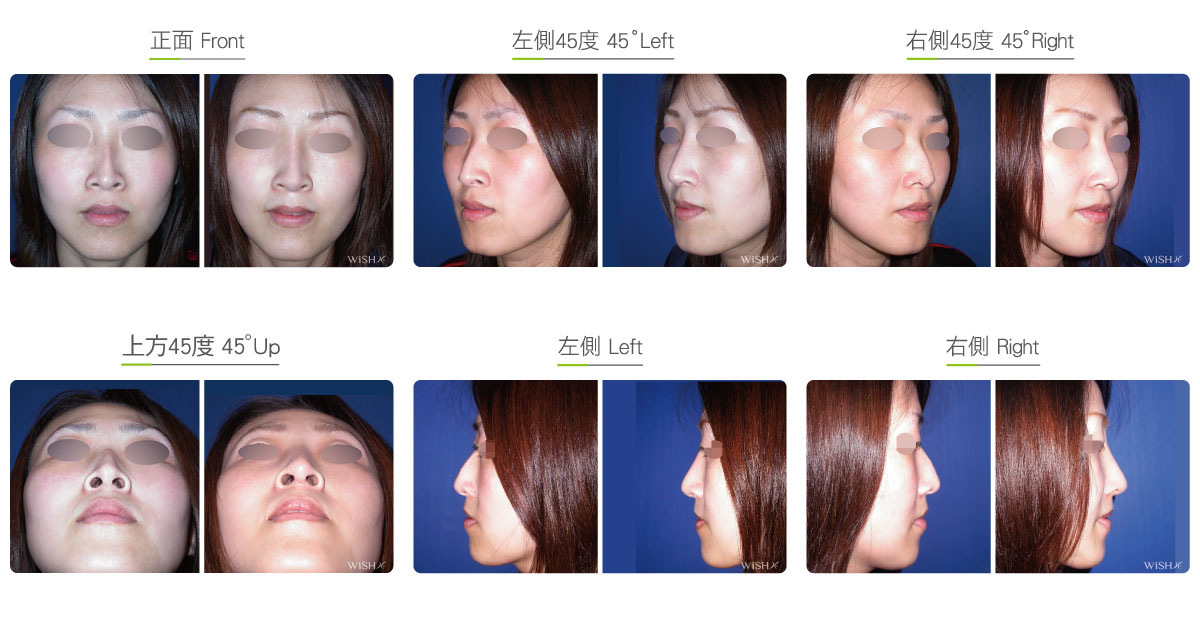
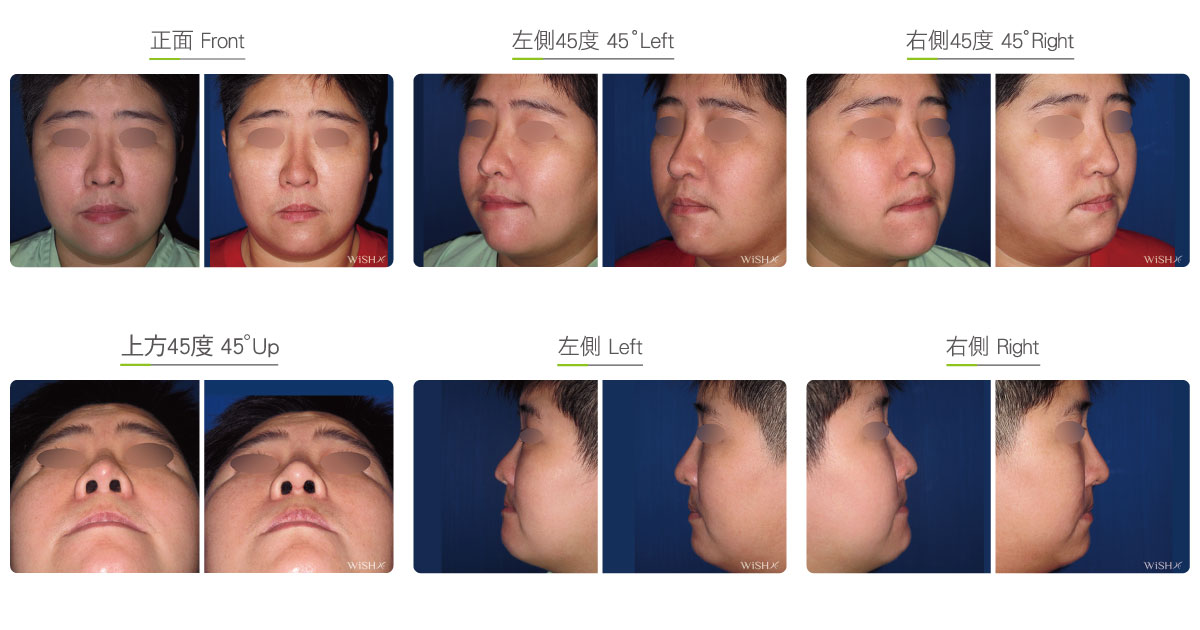
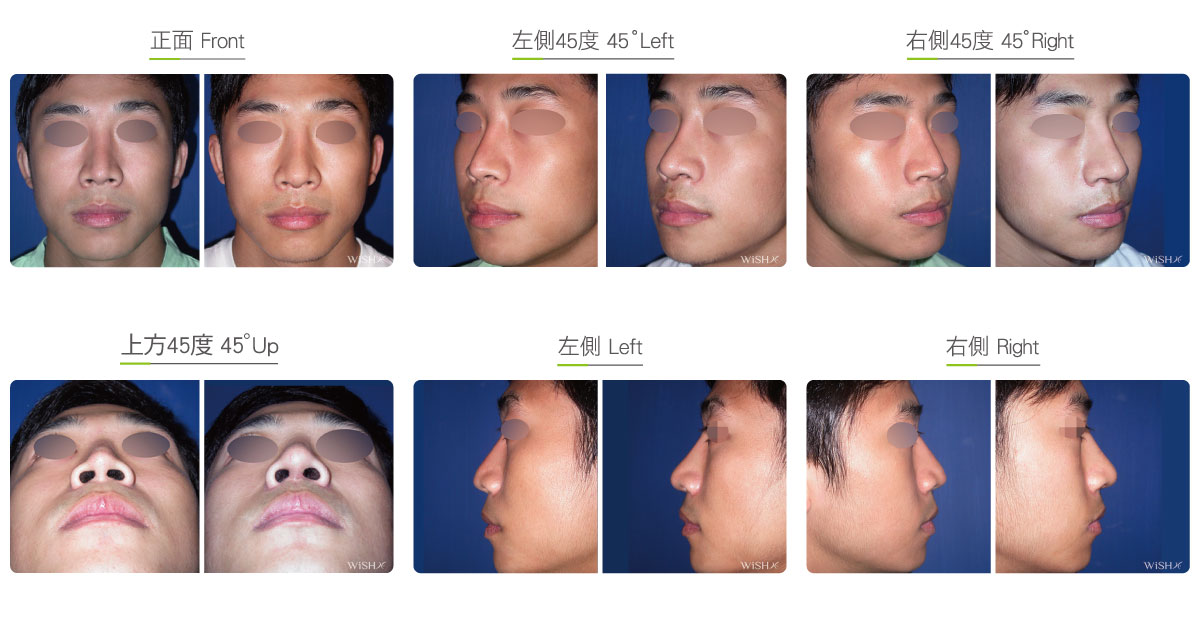
Nasal Fat Padding
The thickness and tension of the nasal tip skin determine the naturalness and durability of rhinoplasty. In clinics, poor conditions of the nasal tip are frequently reported to incur tenser and thinner skin after elongation rhinoplasty, which derives an overtly pointed nasal tip, cartilaginous trace, redness or white spots, and also compromises the stability and sustainability of surgical results. Therefore, it is important to accurately evaluate the distensibility of the nasal tip skin prior to the operation. If it is necessary to reinforce the thickness of the nasal fat, eligible skin tissues are harvested from other body parts, such as the scalp, lower abdomen (groin), or gluteal fold area. In Dr. Chuang’s experience, he considers that the optimal option is the fascia layer at the buttock, whose skin tissues are most abundant and durable. Partial removal of dermal fascia does not affect the appearance or skin evenness over this area, and the incision will be hidden inside the groove of the gluteal folds so that the scar is less likely to be noticed. The removed gluteal fascia, after trimming and scissoring, will be immediately emplaced into the interlayer between the nasal tip skin and cartilage grafts via the open incision at the nasal columella, which adds a layer of autologous fascia at the inner side of the already thinning nasal tip. This not only makes the nasal tip appear round and natural to obviate an exceedingly pointed or pointed shape but also substantially enhances skin resistance to external force friction or compression. Nevertheless, the transplantation of the gluteal fascia to the nasal tip also presents self-resorption, with an absorption rate of approximately 30–50%, which still sustains stable results in the long run.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: At the bottom of the nasal columella and inside the bilateral nostrils
At the depressed gluteal groove (for collection of fascia) - Recovery: 5–7 days
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery
- Do not smoke for 1 week preoperatively
- Avoid smoking and alcohol and impacts or compressions to the nasal tip for 3 months postoperatively, and the clean intranasal wound in the morning and evening every day.
Ideal candidates
- Patients with poor original skin conditions at the nasal tip or an exceedingly thin nasal fat
- Those with a severe snub or upturned nose that requires dramatic elongation of the nasal tip
- Those whose subjective requirement for the elongation of the nasal tip surpasses the tolerability of skin tension
- Those who have undergone multiple rhinoplasties and have very thin tip skin
- Those who have undergone rhinoplasty but need secondary surgery due to the presence of white spots at the nasal tip or pending protrusion
- Those with a deformed nasal tip or nasal tip contracture because of implant protrusion or extrusion from infection
- Those who desire a round and plump nasal tip
Potential complications
- Scarring, poor wound healing, nasal tip inflammation, self-resorption of fascia
- Poor wound healing
- Nasal tip inflammation
- Self-resorption of fascia
Surgical advantages
-
It is able to increase the thickness of the nasal tip skin to render more natural results and texture from rhinoplasty.
-
It is able to obtain a round and stereoscopic nasal tip and elevate the naturalness of the surgical results.
-
It is able to enhance the distensibility and tension of the nasal tip skin to help sustain the prolonged and stable results from rhinoplasty.
-
It is able to prevent nasal tip skin thinning due to revision rhinoplasty.
Surgical drawbacks
-
An additional incision for the collection of facial tissue should be made at other body parts.
-
The nasal tip would become relatively round, plump, or broad.
-
Excess filling of autologous fascia may result in intranasal inflammation or infection.
-
Absorption rate of autologous fascia may be relatively high.