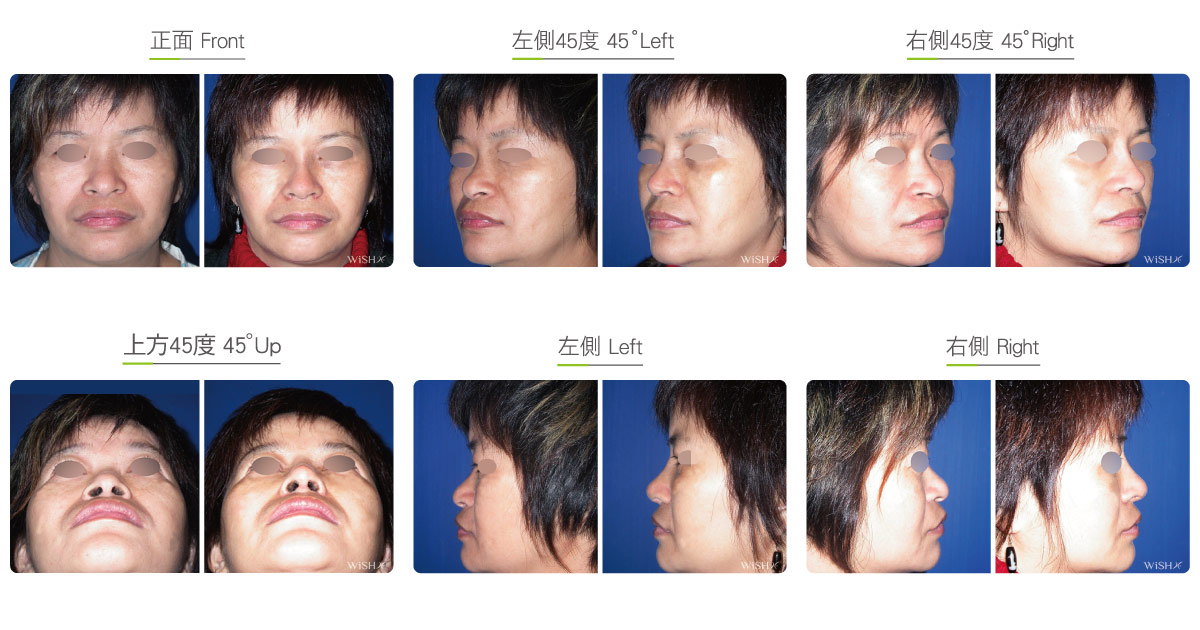
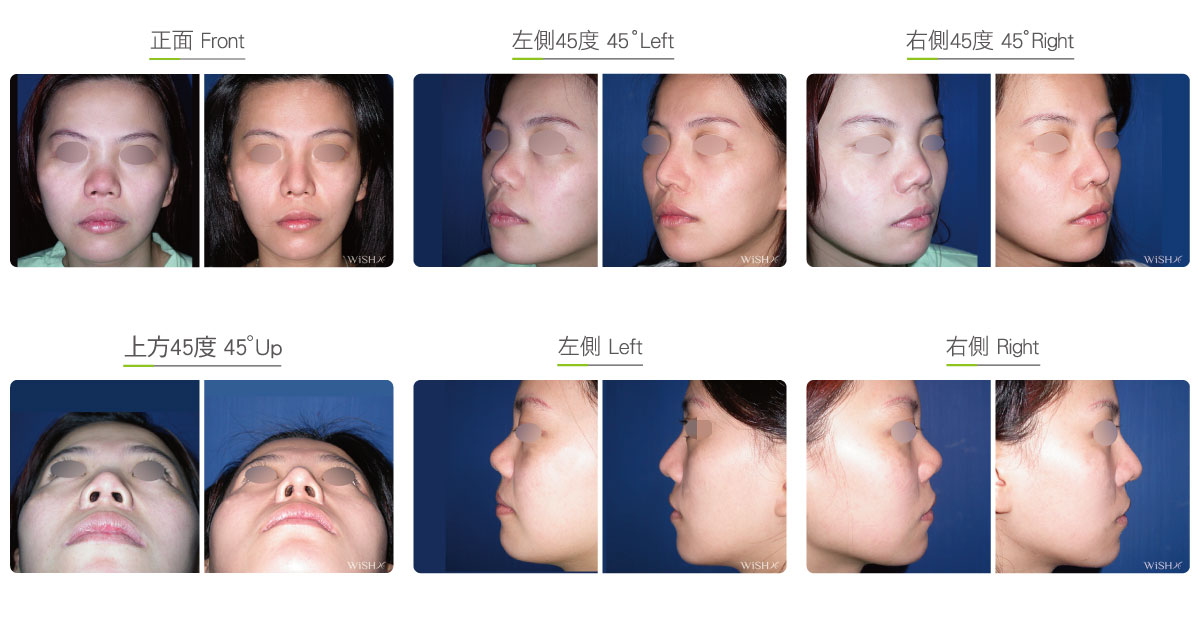
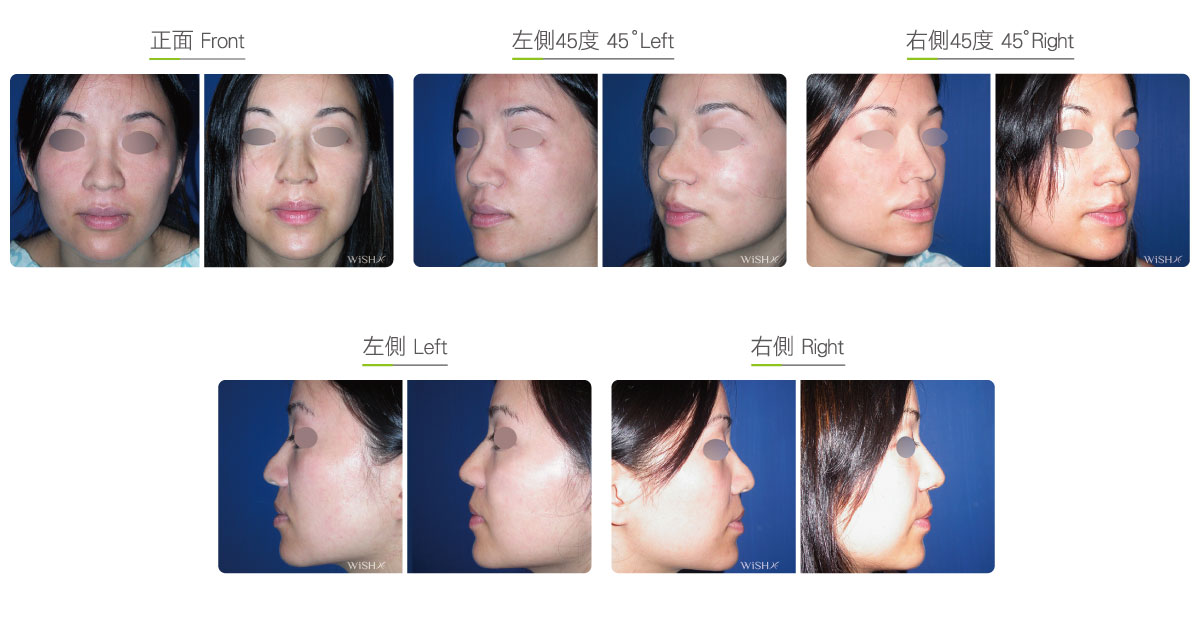
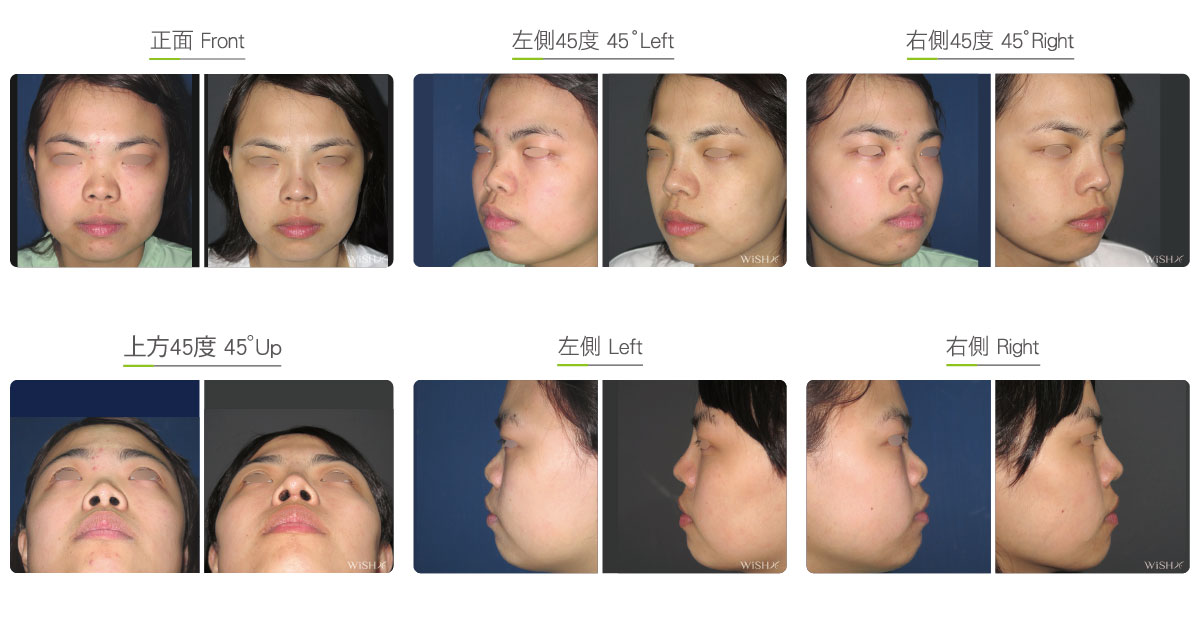
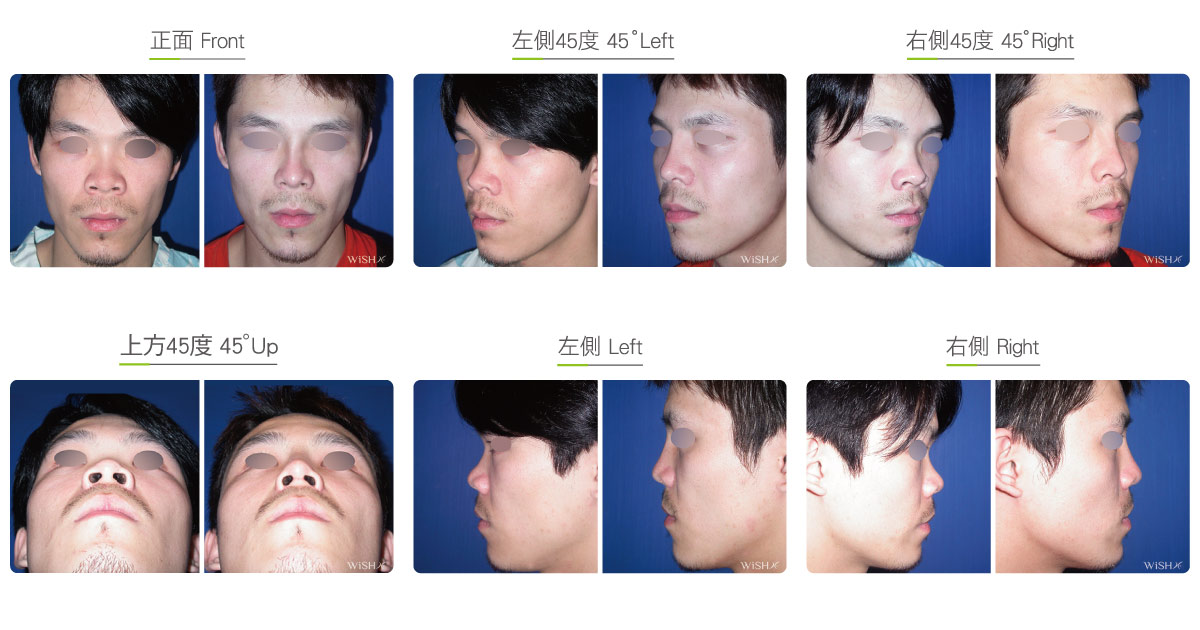
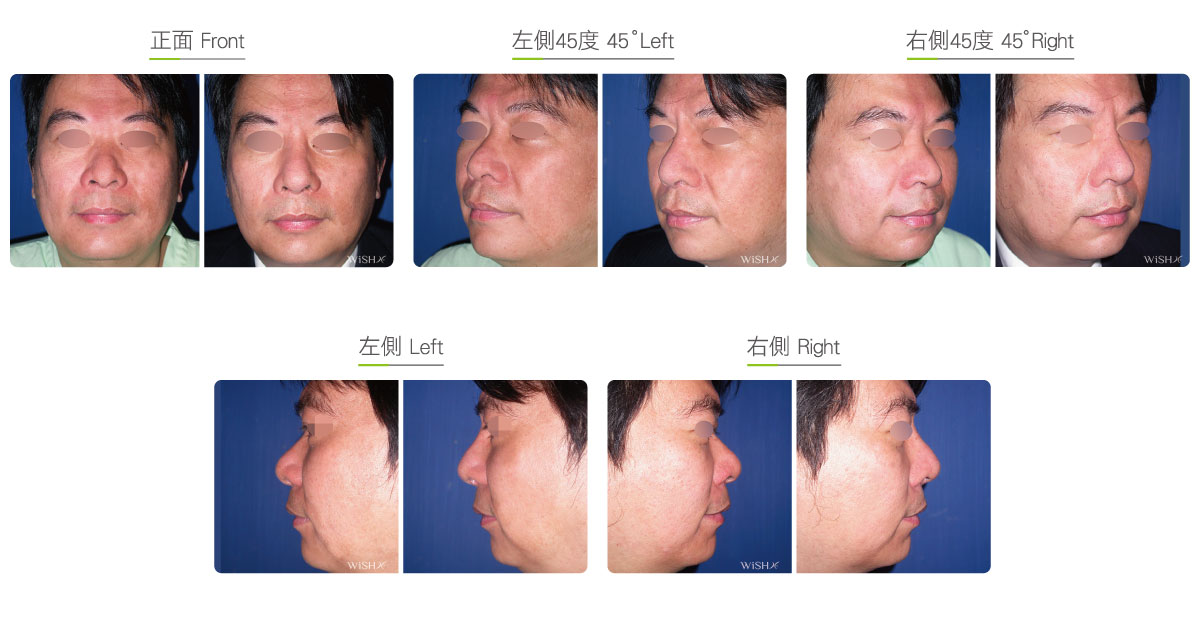
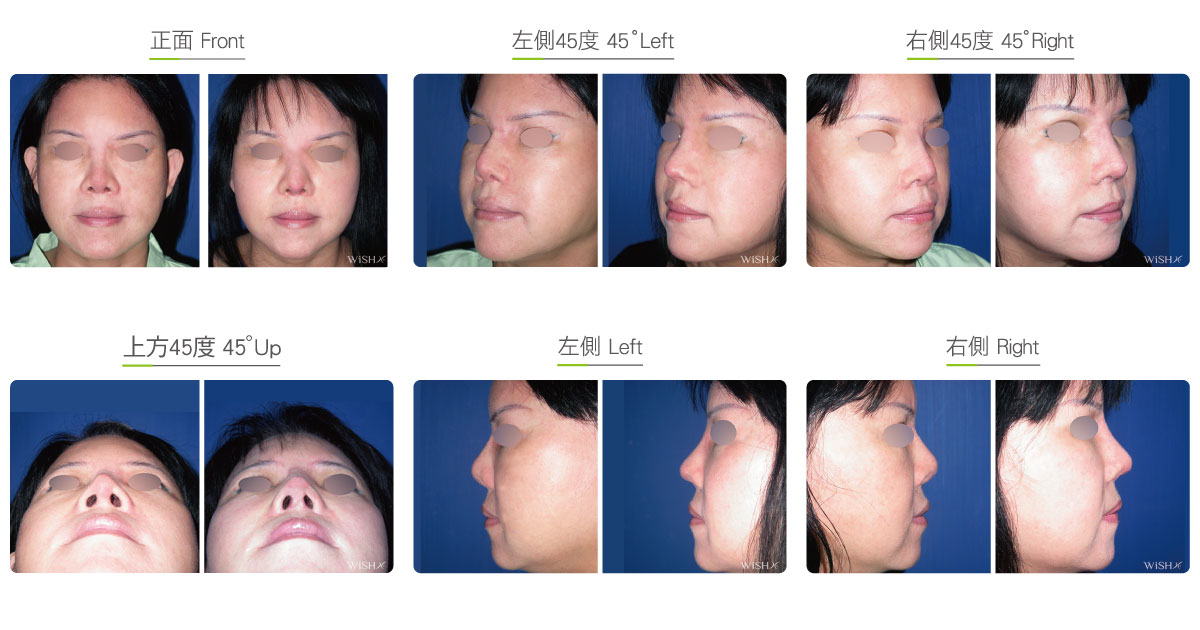
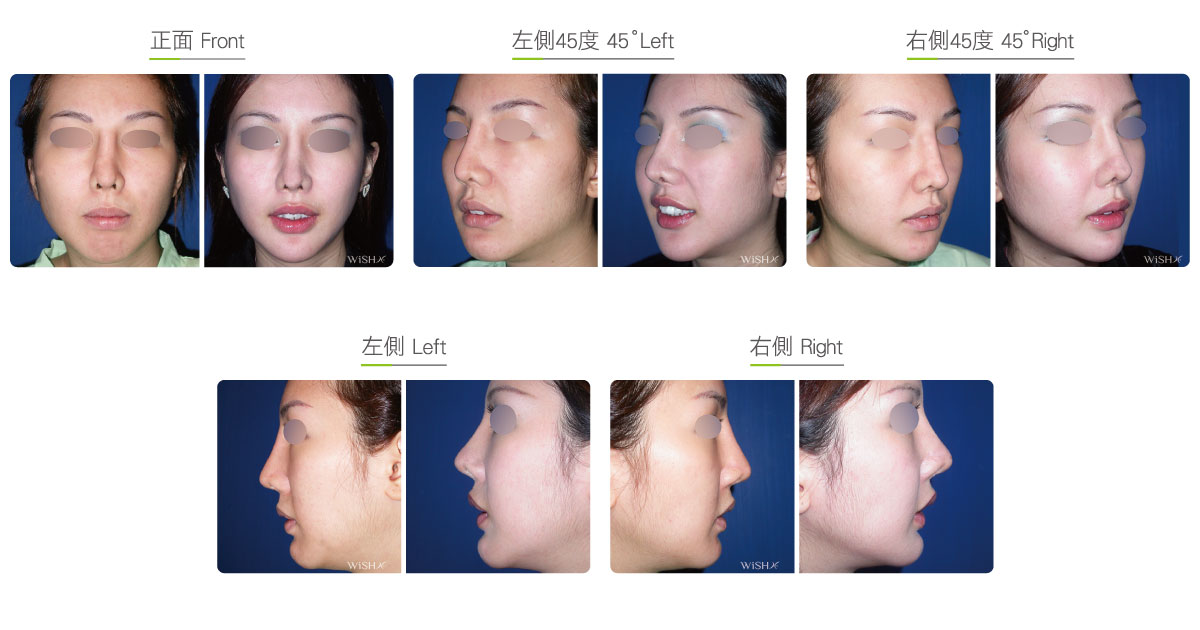
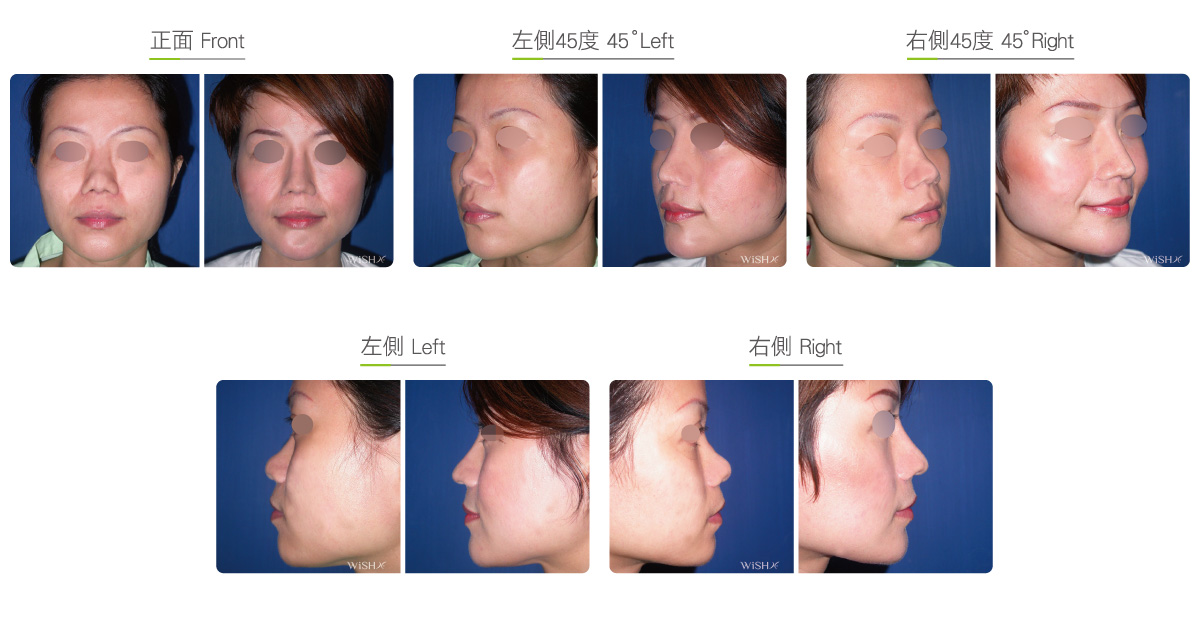
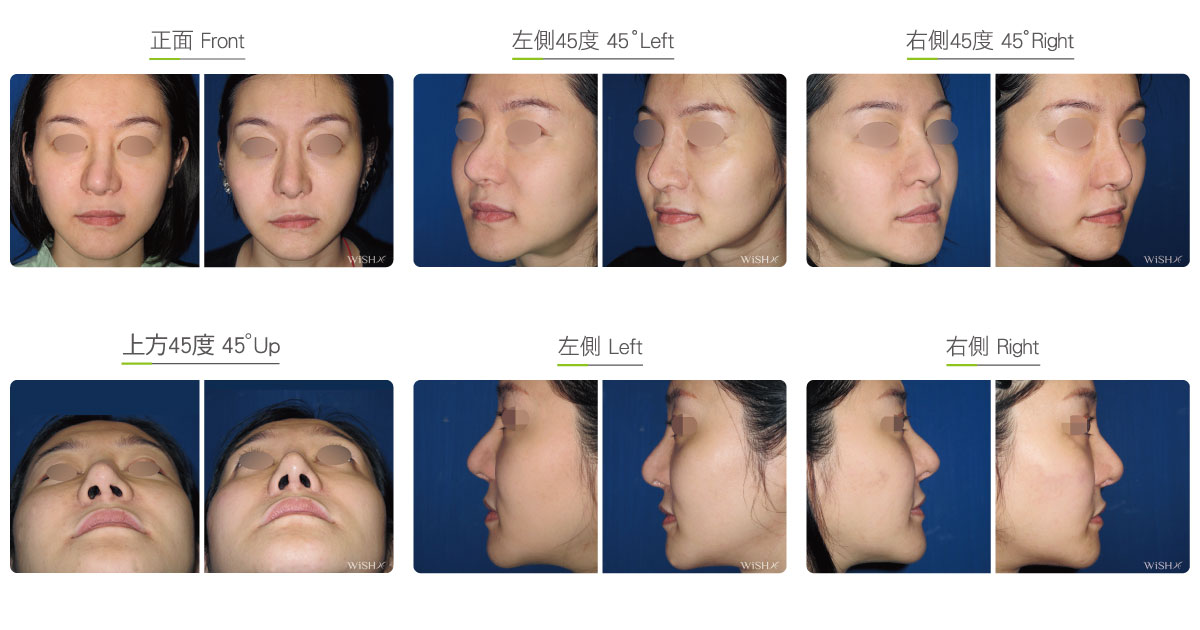
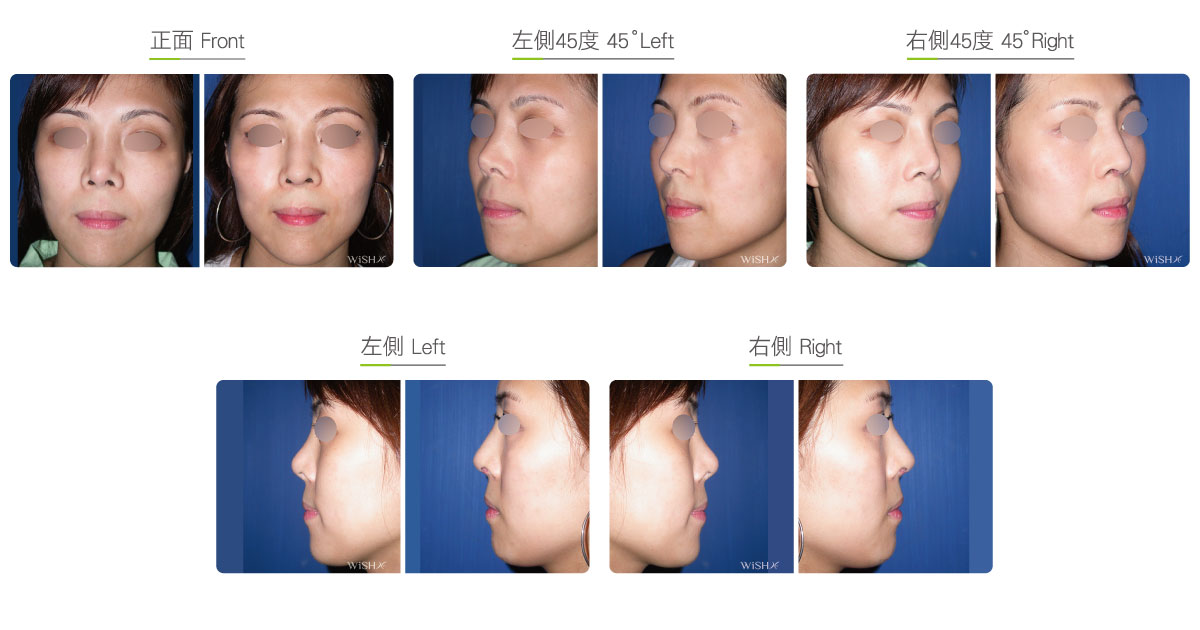
Autologous Costal Cartilage Rhinoplasty
Autologous costal cartilage rhinoplasty is based on viable transplantation and is conducted by processing a segment of the costal cartilage harvested from the patient before it is immediately emplaced inside the nose. Compared with the common open (Korean-style) rhinoplasty, autologous costal cartilage rhinoplasty has the similar surgical method which necessitates to make an open columellar incision, but there is no need to use any artificial prosthesis or nasal septal/auricular cartilage graft because it has a sole requirement of autologous costal cartilage. The site for harvesting the costal cartilage varies along with the gender and rib feature of the patient and is generally at the 6th or 7th rib because it is mostly straight and long enough for the augmentation of the nasal bridge. The incision for the collection of the rib is approximately 3.5 cm and will only leave a thin scar at the anterior chest wall under good wound care. After the costal cartilage is harvested, necessary management will be performed on the rib to prevent curving, including segmentation, straightening, molding, and scoring, and it is then implanted into the nasal bridge, nasal tip, and nasal columella in light of the surgical design. The rib is sculpted into an L-shaped stent to reconstruct an ideal nose shape, and cartilages at multiple sites are then stitched and fixated. Technically as long as the ribs collected are of sufficient length and mass, there will no problem in reconstructing the whole nose.
Dr. Chuang considers that this surgery poses a great detriment to body tissues because the costal cartilage will never regrow after being removed; therefore, it seems to be overdone in applying the costal cartilage for primary or simple esthetic rhinoplasty. Moreover, costal cartilage transplantation has concerns of warping, and approximately 10–15% of patients show different degrees of nasal bridge deviation within 1 year postoperatively, 5–8% of whom will need to undergo revision surgery. Although there are some surgeries currently conducted to break chondrocyte memory and prevent autologous warping, this problem still cannot be completely eradicated. Patients should understand all the advantages and disadvantages of the surgery before making a decision. From the perspective of Dr. Chuang, this surgery is suitable for revision rhinoplasty or traumatic nose reconstruction or for patients with nasal deformity or contracture due to prosthesis infection or removal, and it is also used as the ultimate method to correct a difficult rhinoplasty like excess short nose or saddle nose. In this way, an appropriate plan can be derived that balances surgical risks and patient expectations.
Surgical conditions
Duration
- Type of anesthesia: General anesthesia
- Surgical incision: At the inferior margin of the nasal columella and inside the bilateral nostrils, an approximately 3.5 cm incision at the anterior chest wall (for the collection of the rib)
- Recovery: 7 days
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery (general anesthesia)
- Wear a tape or plaster splint for 1 week postoperatively to stabilize the nasal bridge.
- Avoid smoking and alcohol and impacts to the nasal tip for 3 months postoperatively, and clean the intranasal wound in the morning and evening every day.
- Abstain from eating raw food, seafood, and irritating food or spices for 3 months postoperatively.
- Avoid exposure of the nostrils to dirty water (sea water, swimming pool or sauna water, and hot springs) and close contact with pets and dust mites for 3 months postoperatively.
Ideal candidates
- Patients already undergoing artificial prosthesis implantation but showing foreign body reaction or infection
- Those developing chronic inflammation after repeat rhinoplasty
- Those with nasal tip contracture and deformity due to the removal of an artificial prosthesis
- Those suspected of having chronic prosthesis inflammation or rejection but requiring immediate revision rhinoplasty
- Those with nasal bridge collapse or deformity due to prior trauma (such as a saddle nose)
- Those in need of rhinoplasty reconstruction due to congenital structural defects such as cleft lip and palate
- Those with congenital nasal bone aplasia (such as a severe upturned nose or short nose)
- Those who mentally reject or fear the emplacement of a nasal implant or any foreign body
Potential complications
- Poor wound healing
- Rib autologous warping
- Autologous resorption
- Chest wall scarring
- Pneumothorax / hemothorax
Surgical advantages
-
There is no emplacement of any prosthesis, so no foreign body rejection will occur.
-
The incidence of infection associated with costal cartilage surgery is lower than 1%, which prevents recurrent infection due to prosthesis emplacement.
-
Cartilages are of sufficient mass and strength and can therefore sculpt a projected and definitive nose.
-
The autologous resorption rate of the costal cartilage is lower than that of the auricular or nasal septal cartilage, which helps sustain prolonged stable results.
-
It maximally elongates the nasal tip without any concern of implant extrusion.
Surgical drawbacks
-
An additional scar will be left at the anterior chest wall, which may affect the chest beauty of females.
-
Costal cartilage removal varies in thickness and length due to individual skeletal structure, so the surgical results may also be different.
-
Despite preventive treatment such as straightening and scoring, the rib may still develop gradual deviation, with the average incidence at approximately 10–15%.
-
Complications such as pleural perforation or even pneumothorax/hemothorax may occur on the collection of ribs, and postoperative pain is also more obvious.
-
The removed rib will not regrow, so resistance to impacts may be poor.
-
The nasal tip feels relatively hard, and future motion may be limited.
-
The operation may take a long time so it is expensive.