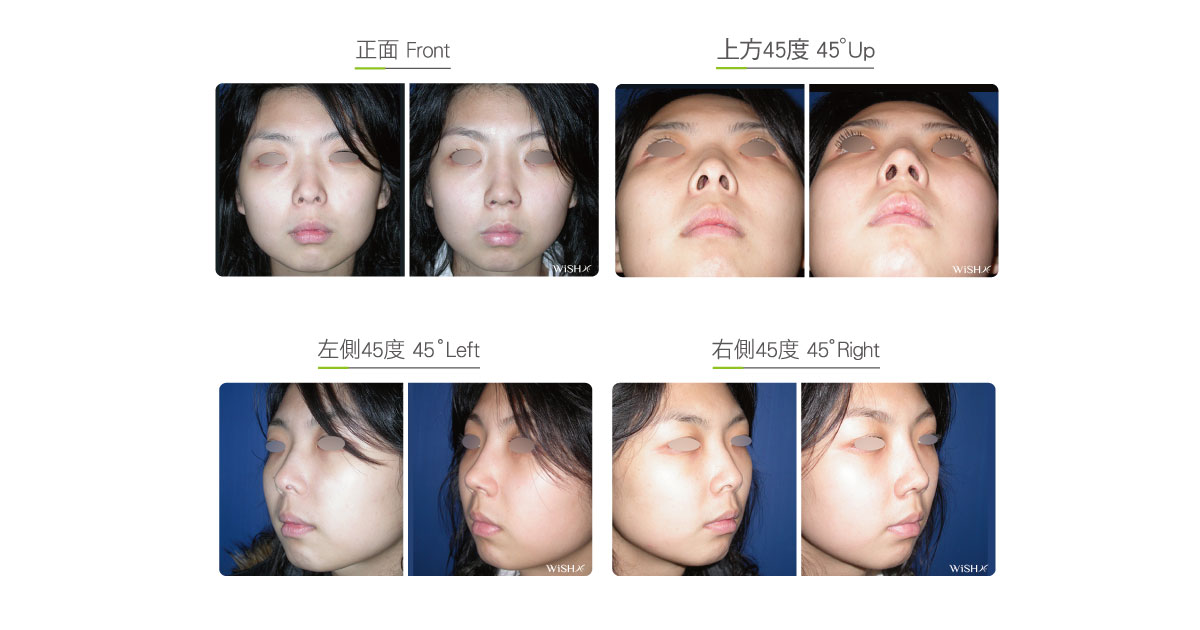
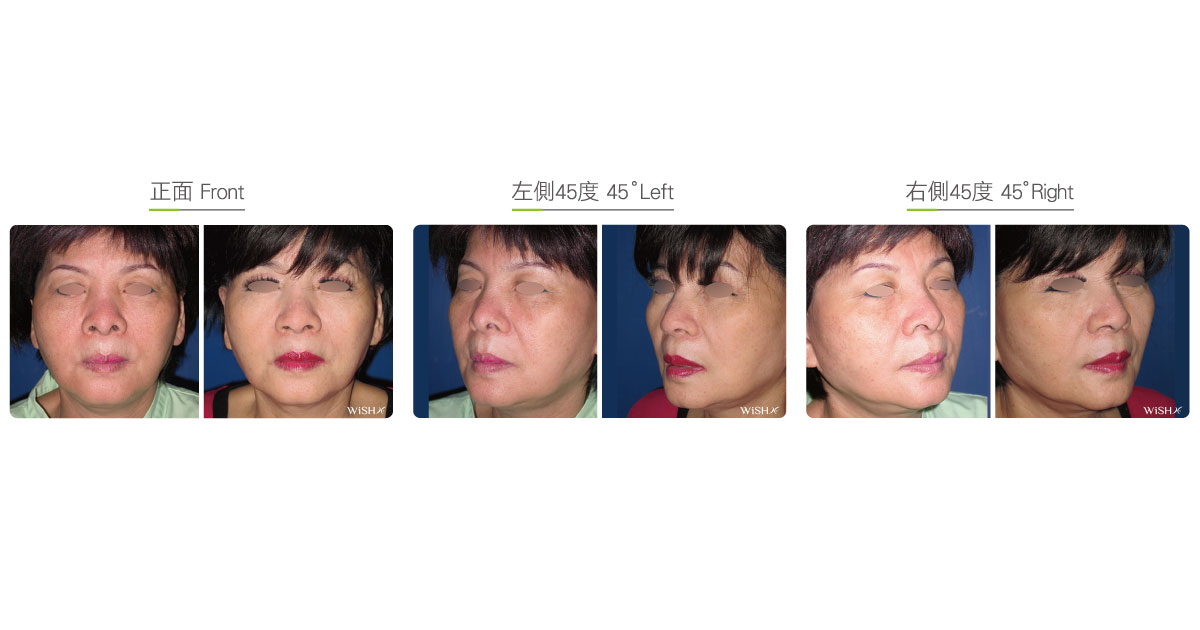
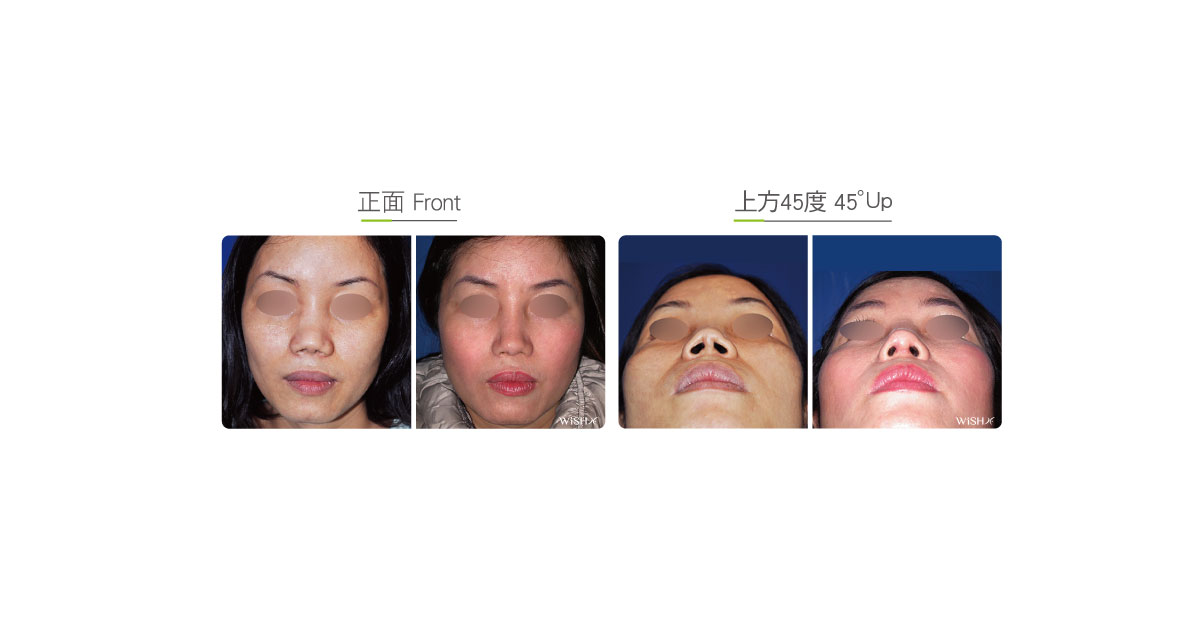
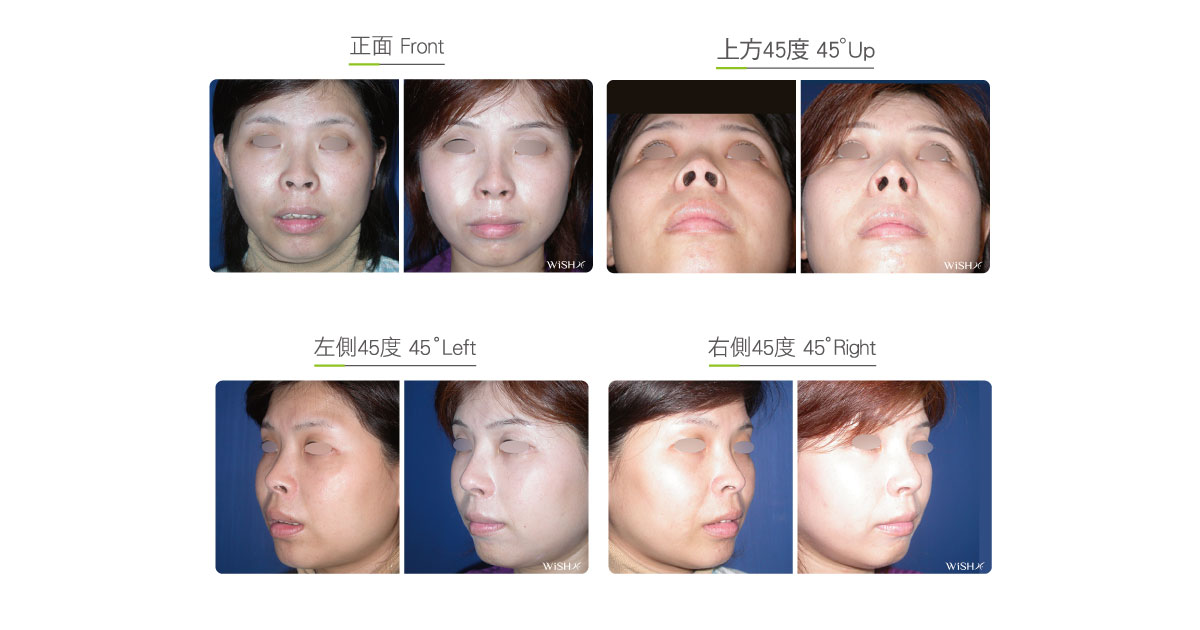
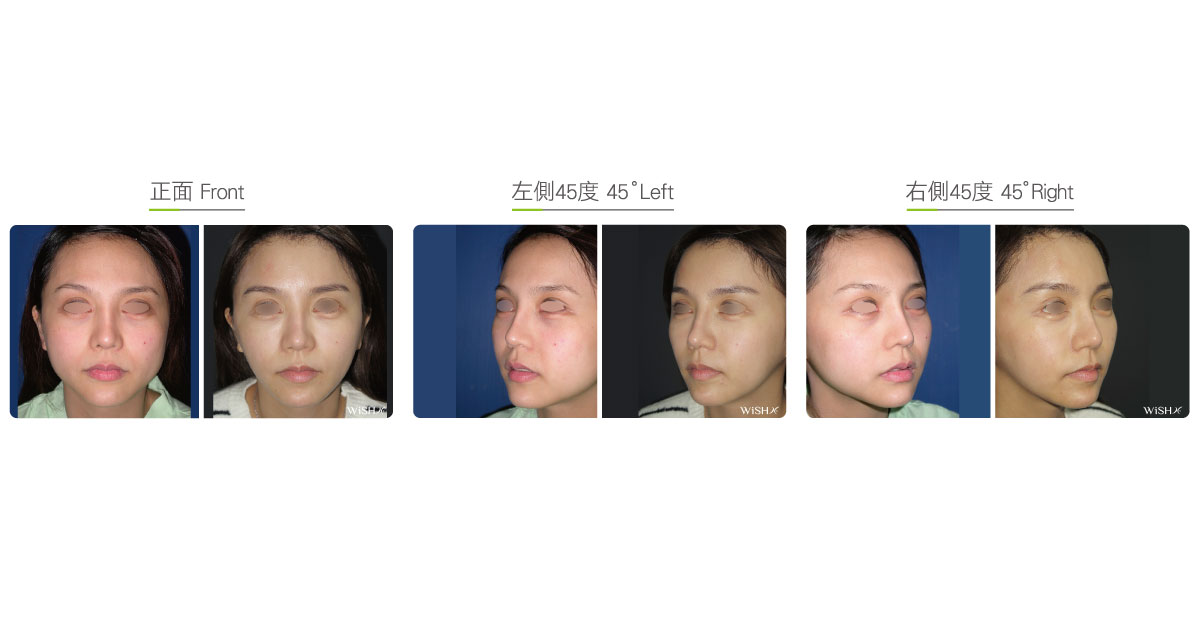
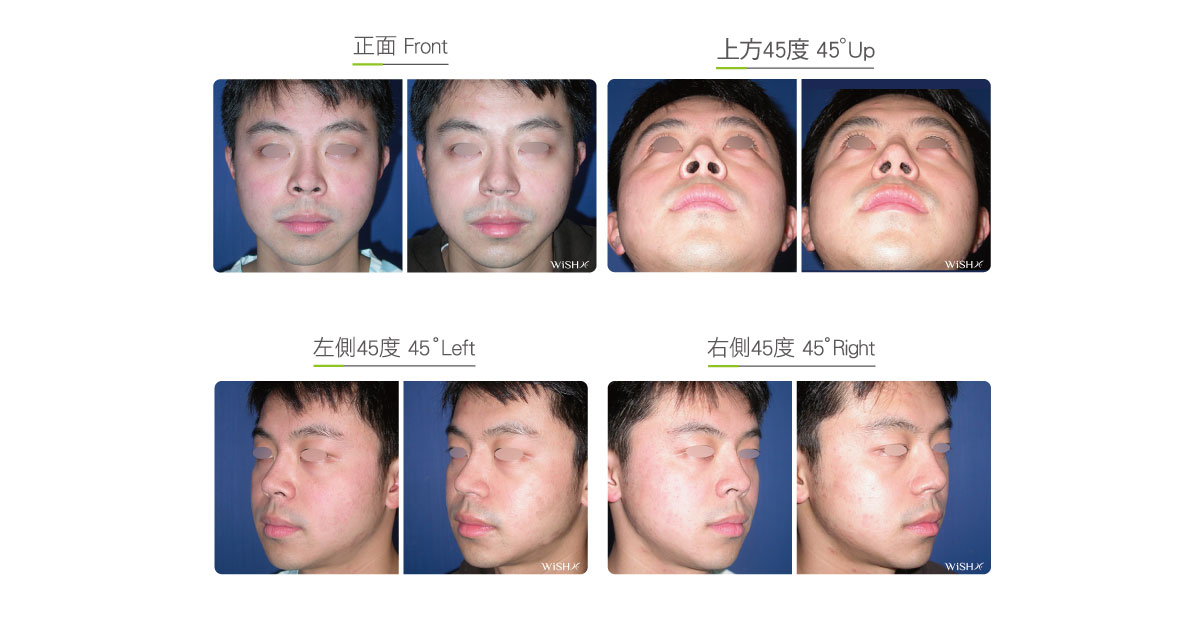
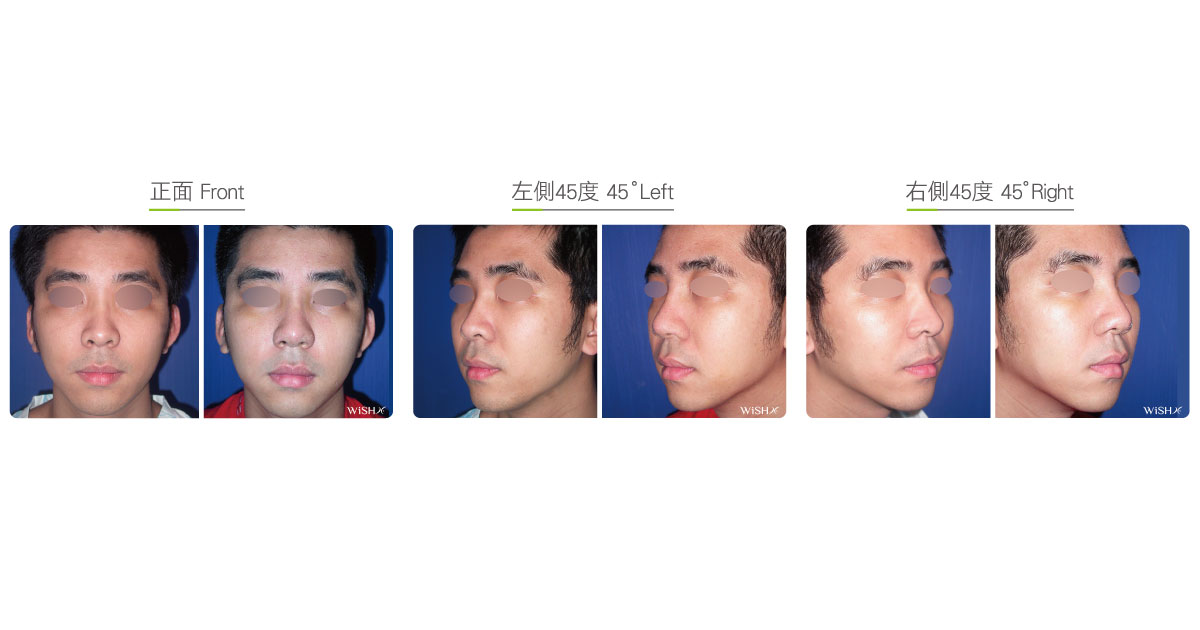
Nostril Exposed Correction
It is also called “alar rim augmentation”. Clinically, there are two common causes for nostril exposure. One is attributed to the alar and nostril slanting upward due to an exceedingly short or upturned nasal tip (short nose), which could be modified by open (Korean-style) rhinoplasty or nasal tip elongation surgery (open tiplasty). The other is attributed to simple alar rim insufficiency or retraction, leading to overt exposure of the nostrils from the frontal view, and gives the top of the nostril the appearance of a triangle. However, because the nasal tip angle and length of some patients are still within the normal range, the problems cannot be fully corrected even by open rhinoplasty or upturned nose correction, so further alar rim augmentation or repair is necessary. At present, there are no standards for defining nostril exposure. However, if it is beyond the subjective acceptance or even to the resent of patients, nostril exposure correction is considered. This surgery is mainly aimed to fill the skin defects of the superior alar rims and is conducted by collecting the auricular cartilage with a skin structure by “composite auricular cartilage transplantation,” which is then emplaced at the medial side of the nostril via an incision at the inner margin where the nostril is exposed to extend the alar defect outward and posteriorly via the mass and volume of the auricular cartilage and achieve the ultimate objective of reducing the nostril exposure. Nevertheless, because the regional skin is difficult to stitch and very tight and the autologous absorption of the auricular cartilage is relatively high, Dr. Chuang mostly conducts certain degrees of “over-transplantation.” Patients will feel lumps or bulging at the medial side of the nostrils during the early postoperative period, which gradually become smooth and soft due to the partial absorption of the cartilage within 3–6 months and appear natural and normal. In addition, if the patient has a concurrent enlarged ala nasi and nostrils, alar reduction will be simultaneously performed to garner better results.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: Medial skin at the defective area of the ala rims (inside nostrils)
- Recovery: 3–5 days
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery
- Do not smoke for 1 week preoperatively
- Avoid smoking and alcohol for 3 months postoperatively; clean the intranasal wound in the morning and evening every day, and avoid picking the nose with fingers.
Ideal candidates
- Patients with normal width of ala nasi but obvious nostril exposure due to alar skin deficiency
- Patients with nostril exposure due to congenitally exceedingly thin alar tissues
- Those with a normal nasal tip length and angle but with nostril exposure
- Those whose nostril exposure cannot be improved by open rhinoplasty or short nose correction
- Those who require completely concealing nostrils
Potential complications
- Poor wound healing
- Cartilaginous absorption
- Masses inside the nostrils (temporary)
- Incomplete correction
Surgical advantages
-
The correction of nostril exposure by concurrent cartilage and skin transplantation offers stable and lasting results.
-
Alar repair is conducive in beautifying the relative ratio between the nasal tip and nostrils.
-
The surgery is able to completely solve the defects of congenital alar retraction.
-
The surgical results are stable and do not result in any deformity.
Surgical drawbacks
-
Temporary thick skin or lumps may develop inside the nostrils.
-
For patients with a congenitally short nose or upturned nose, open rhinoplasties or tiplasties should be performed to achieve complete improvement.
-
There might be an autologous absorption at the area of the ala nasi where the auricular cartilage is transplanted.