Calf Muscle Resection
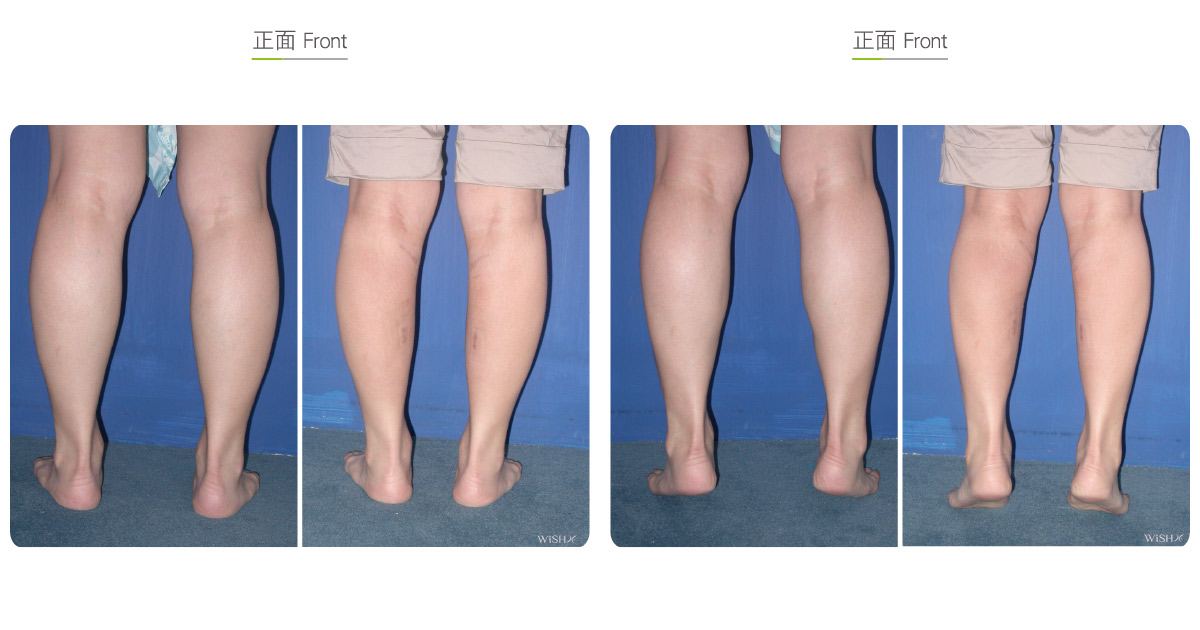
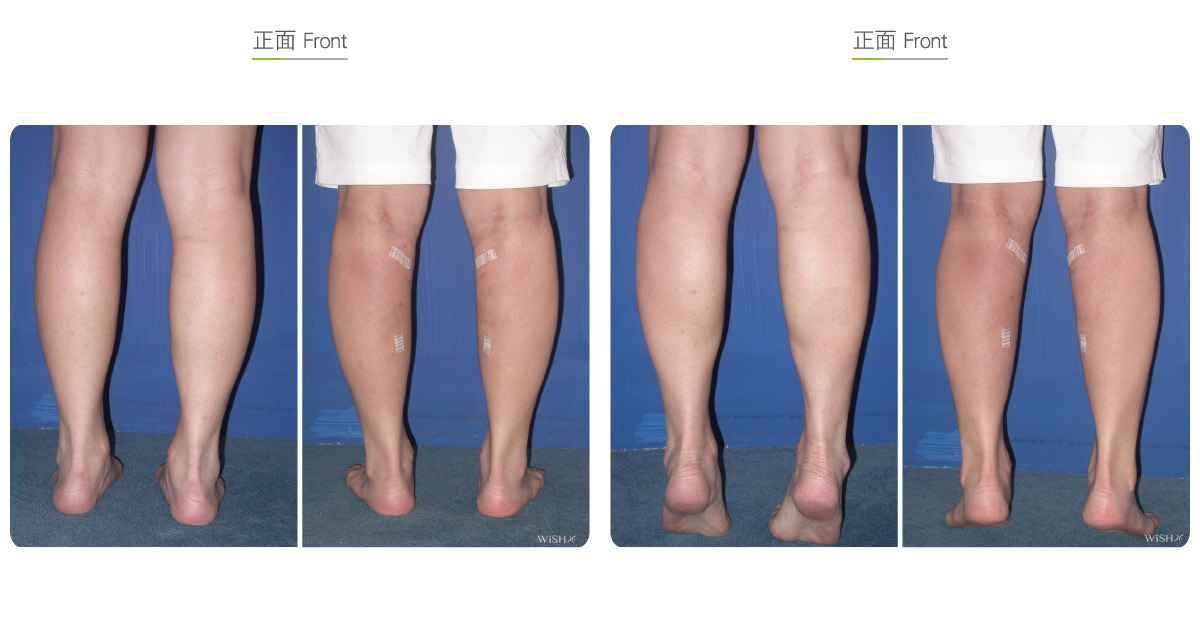
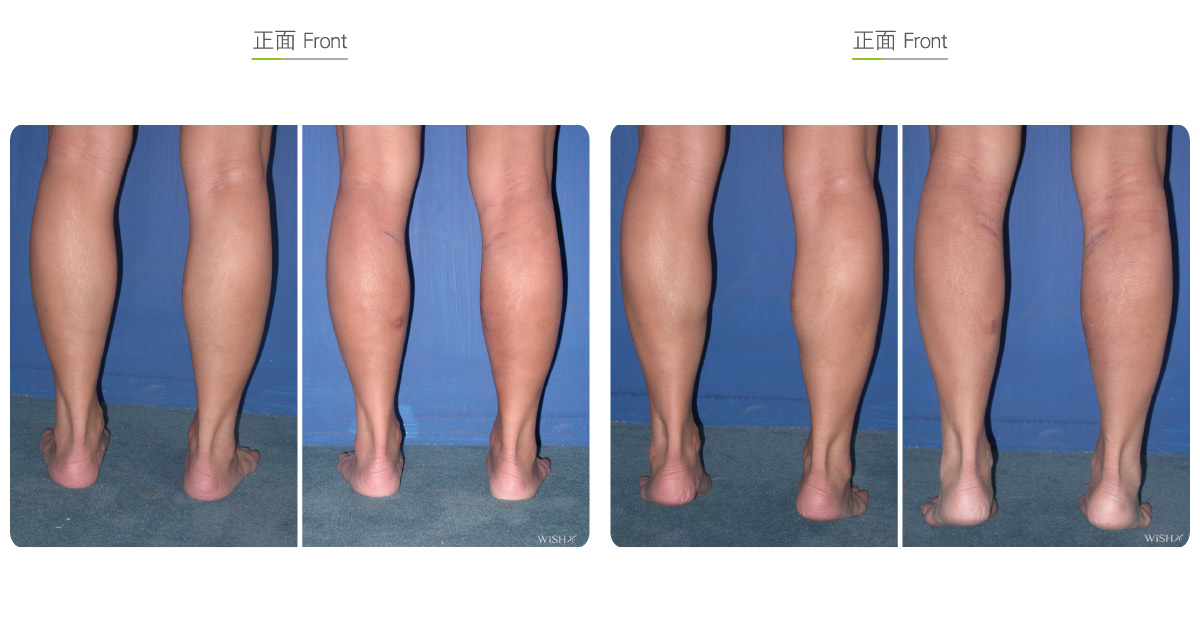
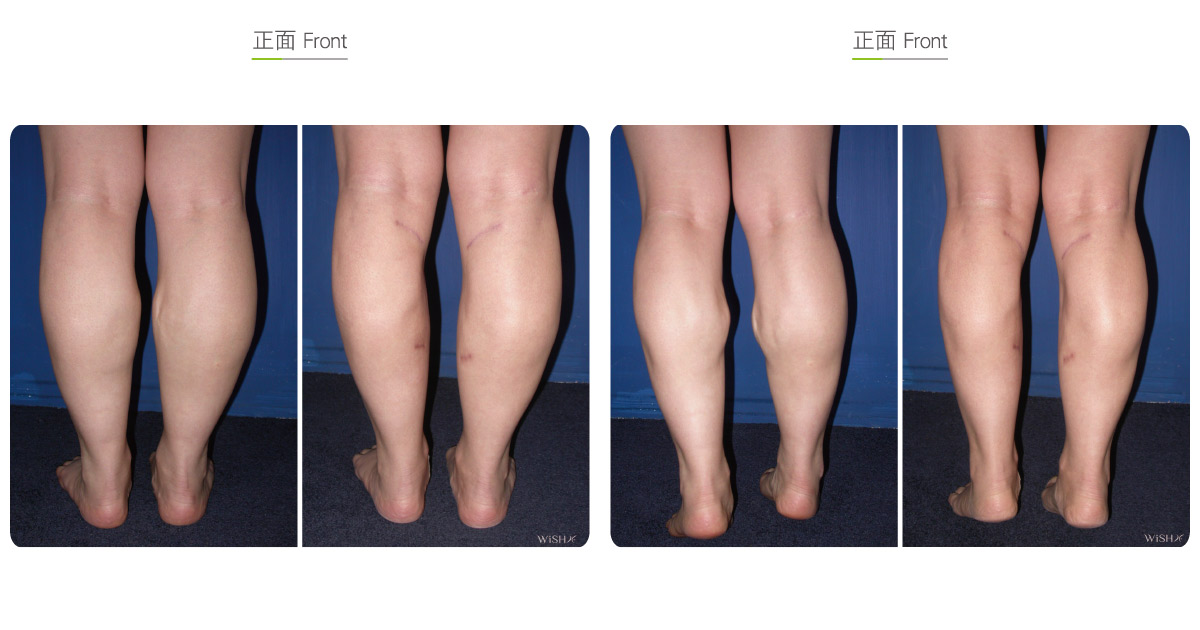
This method targets purely congenital muscular calf bulkiness, elephantine legs susceptible to edema, thick legs with overtly developed lateral gastrocnemius muscles, or thunder hypertrophy that cannot be effectively reduced by nerve blocking. It involves the direct removal of the medial or partial lateral gastrocnemius muscle to decrease the muscular volume and achieve distinct leg slimming. A 4–5-cm incision is made at the superior calf close to the patellar fossa. Next, Dr. Chuang utilizes an endoscope to separate the skin from calf muscles and ligates the nerve and blood vessel governing the muscles. Then, the calf muscle is resected via an inferior small incision and removed from a superior incision. If the patient has concurrently thick fat, calf liposuction is simultaneously conducted to enhance the leg slimming result. Patients should wear compression stockings for 3 months postoperative to accelerate leg slimming, which may be achieved within 3 months postoperatively.
This surgery is performed for the maximal reduction of calf muscular volume to attain an extreme leg slimming effect. Different from nerve blocking that makes the muscle atrophy but still in place, muscle resection effectively decreases the leg circumference by 3–4 cm and is the most effective calf reduction surgery. Postoperative recovery is slower but similar to that in nerve blocking as patients experience a temporary change in gait and step after the surgery and feel slightly pain, which gradually becomes normal within 2 weeks. After then, patients do not feel the difference of muscle removal in daily activities and work. Nevertheless, because the surgery is relatively extensive and destructive to tissues and muscles removed do not proliferate in the future, muscular endurance necessary for leg activities are greatly affected, and patients may be unable to perform strenuous activities or activities in need of explosive power or requiring endurance. In a minority of obese patients, this surgery increases the weight bearing load of knees, thus causing premature or excess degeneration of the knee joint. Additionally, for some patients with congenitally less straight or centered legs, the surgery exacerbates the drawbacks of an O-shaped leg. Dr. Chuang advises patients to consider individual work and exercise patterns before undergoing the surgery.
Surgical conditions
Duration
- Type of anesthesia: General anesthesia
- Type of incision: A 4–5-cm incision near the popliteal fossa
- Recovery: 5–7 days
- Removal of stitches: 7–10 days
General instructions
No food and water on the day of surgery
- Avoid running or wearing high heels for 1 month postoperatively to prevent falling due to an unsteady gait.
- Do not run fast, jump, or perform other strenuous activities of the calf for 1 month postoperatively.
- Wear compression stockings for 3 months postoperatively to accelerate the calf slimming results.
- Decrease the weight-bearing work or activities of the leg in the future to prevent excess weight load on the knees.
Ideal candidates
- Patients with a congenitally bulky lower leg
- Those with an elephantine leg predisposed to chronic edema
- Those with a thick leg typical of exceedingly developed calf muscles
- Those who have received a Botox injection or nerve blocking surgery but attain indistinct results
- Those who aspire for extreme leg slimming results
Possible complications
- Inadequate calf muscular tolerance
- Scar proliferation
- Excess weight load on the knee joint
- Nerve injury (difficulty in raising the feet)
- Calf depression
Surgical advantages
-
The leg slimming effect is most obvious.
-
Results are permanently stable and consistent.
-
There is rare compensatory hypertrophy when the muscle is removed.
-
It is able to partially improve the constitution of lower leg edema.
Surgical drawbacks
-
There is a temporary lower leg disability, and the pain is relatively obvious.
-
The postoperative scar can be noticed.
-
The calf muscle strength and tolerance may be inadequate.
-
Obese patients may present prematurely degenerative knee joint problems.
-
Defects of an O-shaped leg may be aggravated in patients whose legs are not straight.
-
Excess muscle resection may lead to calf depression or a deformity.