Selective Nerve Blocking (Calf Neurectomy)
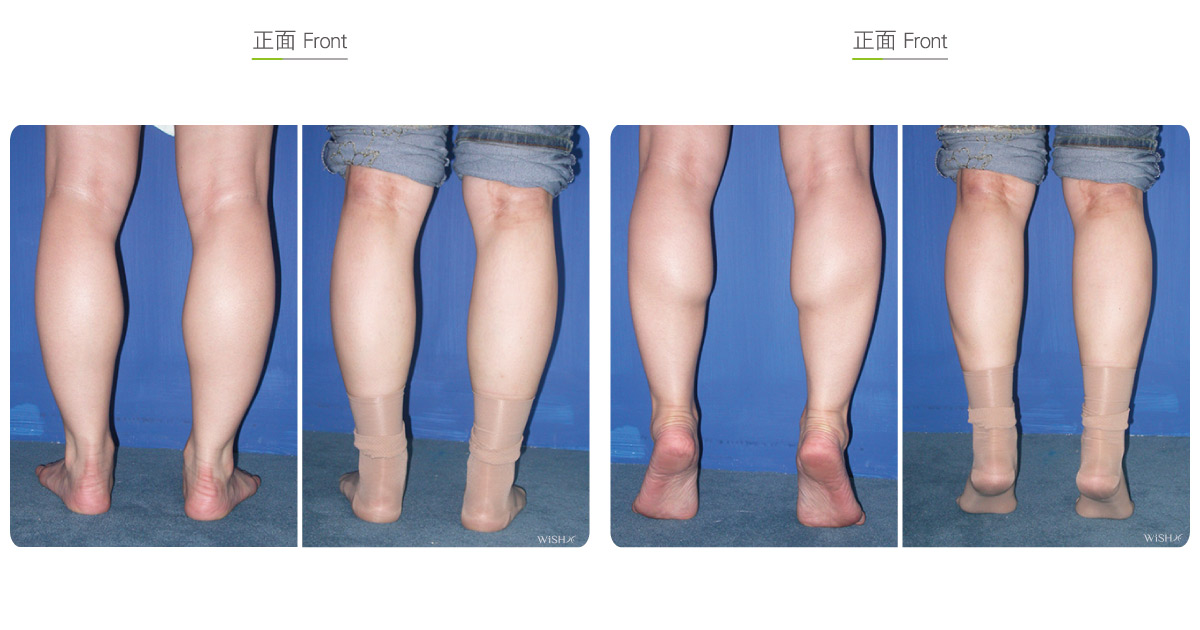
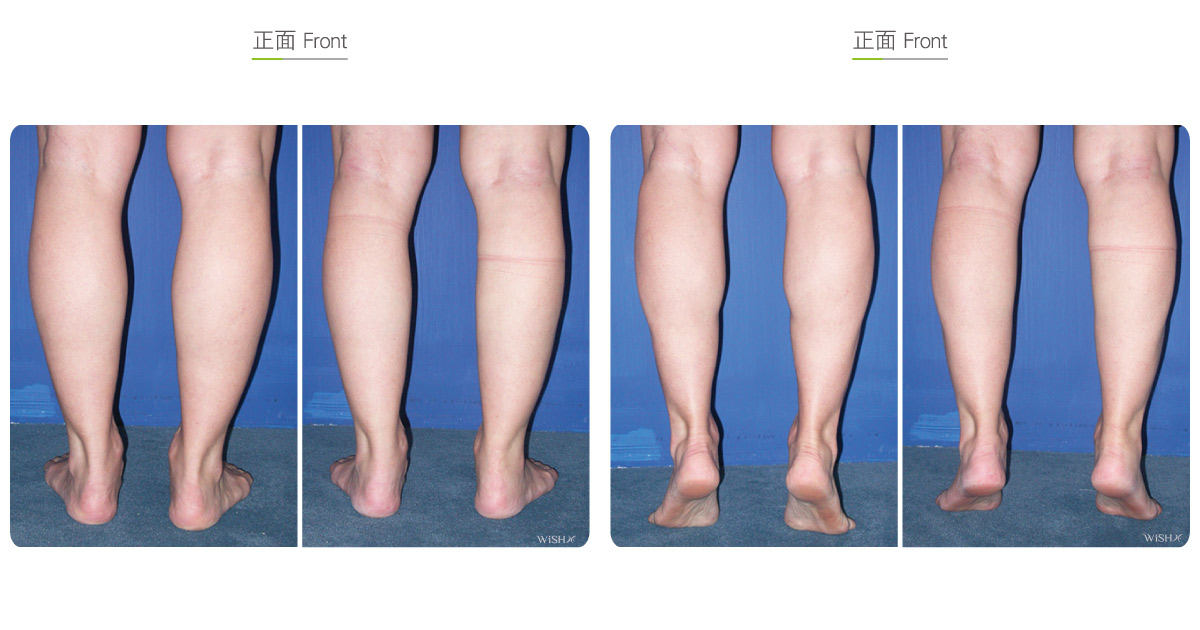
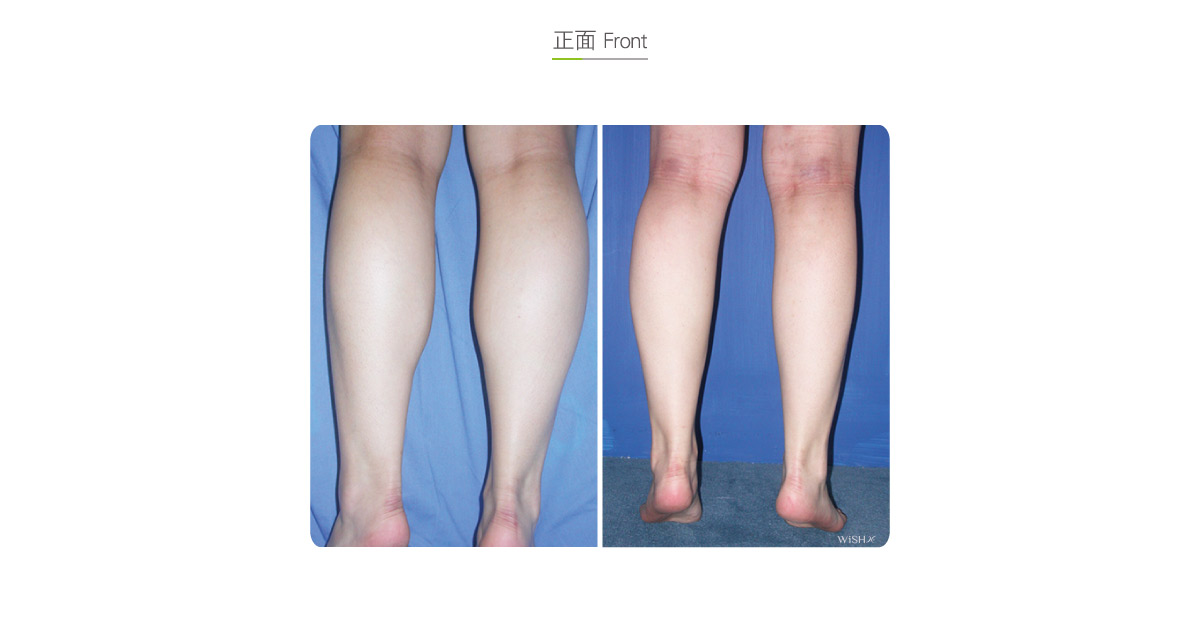
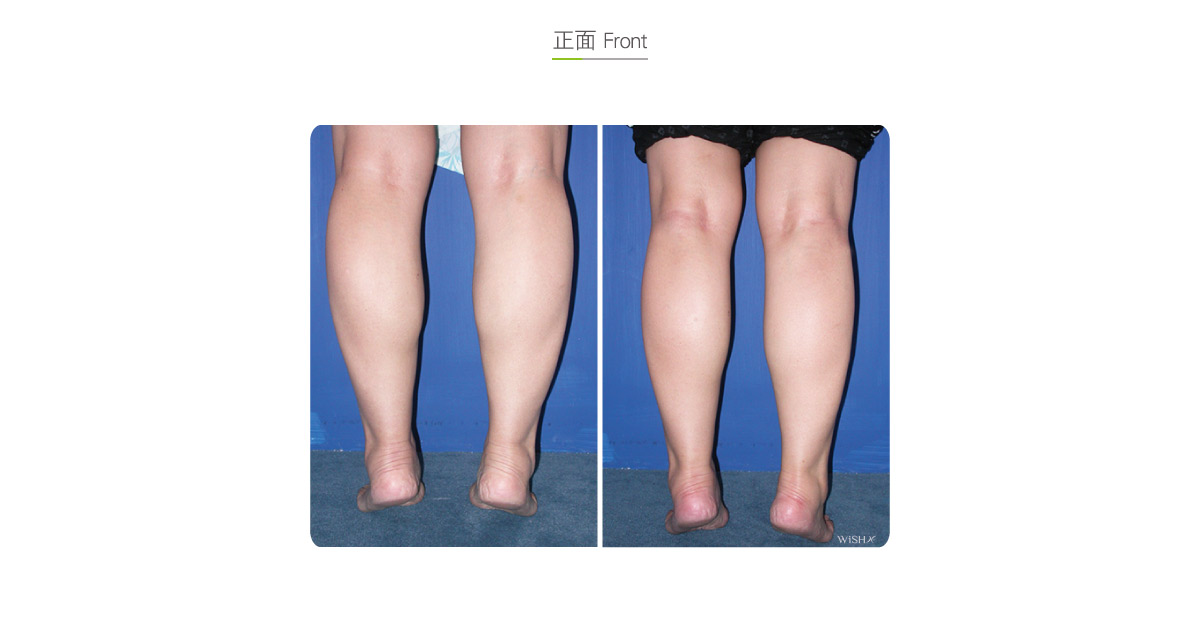
This surgery, also called calf neurectomy, blocks the nerve governing the calf muscle to make it waste away naturally and shrink, thus achieving the ultimate purpose of calf reduction. Anatomically, the lower leg contains three primary muscles. The deepest muscle is the soleus, which governs the major flexion and extension, as well as the motion strength, of the calf (70%), but it does not directly contribute to the leg shape or appearance. Theoretically it should be reduced by any treatment; otherwise, the leg will be unable to exert forces or even support the body weight. Above the soleus and close to the skin surface are two other muscles, namely the medial gastrocnemius muscle and lateral gastrocnemius muscle, accounting for 30% of calf functions, whose role is to facilitate the explosive power, stamina, and foot steadiness. If overtly developed or hypertrophic, muscles would become prominent to induce thunder hypertrophy (medial gastrocnemius muscle hypertrophy), an O-shaped leg (lateral gastrocnemius hypertrophy), or even thick legs (bilateral gastrocnemius hypertrophy). Moreover, thunder hypertrophy is the most common disturbance in females and is the site that is most frequently treated by calf nerve blocking.
It is a minimally invasive surgery. First, a 1.5-cm incision is made at the popliteal fossa at the back of the kneecap. Dr. Chuang identifies the motor nerve branch governing the medial gastrocnemius muscle under the assistance of a microscope, and after the governed muscle is identified by an electric nerve stimulator, the nerve is fully severed and ligated. Thus, the muscle no longer receives stimuli from the nerve and gradually atrophies within 1 month, thus slimming the leg and resolving thunder hypertrophy. Patients have a slow walking pace, are unable to run, and have an unsteady gait (such as a penguin step) or other temporary discomforts due to the instant lack of auxiliary support of the medial gastrocnemius muscle for 1 week postoperatively; they gradually regain the normal gait after approximately 1 week. Moreover, patients should wear compression stockings for 2 months postoperatively to help dissipate the swelling and accelerate the leg slimming effect, with the final results able to be determined within 3 months at the latest.
This surgery is mainly applied to improve the thunder hypertrophy incurred by hypertrophy of the medial gastrocnemius muscle and sculpts the leg shape to make the calf slender and free of a prominent muscular appearance. Despite the medial gastrocnemius muscle becoming atrophic due to a loss of nerve control, there are still certain muscles left, so the slimming effects are confined by congenital conditions, with average reduction of the leg circumference at approximately 1.5–2 cm. However, the explosive power and muscle endurance of the calves of the patients may be undermined, so they must be prohibited from performing strenuous or prolonged activities initially after surgery; otherwise, the residual calf muscles may get hypertrophic in the near future. Moreover, patients should also try to avoid wearing high heels in the long term or performing leg activities to temper the calf muscles in daily life; otherwise, it may incur compensatory hypertrophy of other muscles, resulting in the recurrent bulk appearance of the calf.
Surgical conditions
Duration
- Type of anesthesia: General anesthesia
- Type of incision: A 1.5-cm incision at the posterior knee (popliteal fossa)
- Recovery: 5–7 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Avoid running or wearing high heels for 1 month postoperatively to prevent falling due to an unsteady gait.
- Do not run fast or jump or perform other strenuous calf activities for 1 month postoperatively.
- Wear compression stockings for 2 months postoperatively to accelerate the calf slimming results.
- Decrease the weight-bearing work or activities of the leg to prevent muscular compensatory hypertrophy in the future.
Ideal candidates
- Patients with muscular calf hypertrophy
- Those with medial calf prominence such as thunder hypertrophy
- Those who are unable to slim their legs by a Botox injection
- Those who are impatient in repeated Botox injections but ask for the permanent solution
- Those who objectively feel that their calves are too bulky
Possible complications
- Inadequate calf endurance
- Compensatory hypertrophy (recurrent)
- Scarring
- Results short of expectation
Surgical advantages
-
It slims the legs and beautifies the leg shape.
-
It is minimally invasive and quite safe.
-
The incision is small and less likely to leave a scar.
-
It saves the inconvenience and costs of repeated Botox injections.
-
It makes no obvious influences on daily activities postoperatively.
Surgical drawbacks
-
The degree of muscle reduction cannot be quantified.
-
It may induce calf compensatory hypertrophy.
-
Results may be unobvious for patients with congenitally plump or thick legs.
-
It may affect the explosive power and muscle endurance of the calf.
-
The degree of calf slimming is unpredictable due to the individual skeletal framework and muscular thickness.
-
The reduction of calf circumference is limited.