Wire Scalpel (Combined with Autologous Fat Grafting)
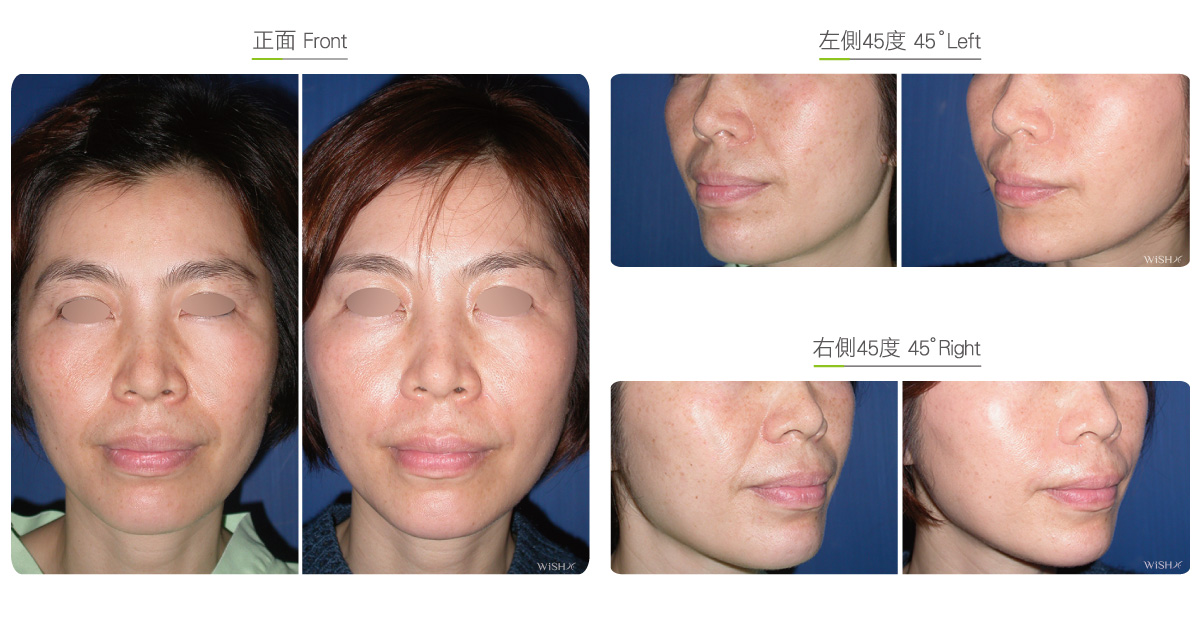
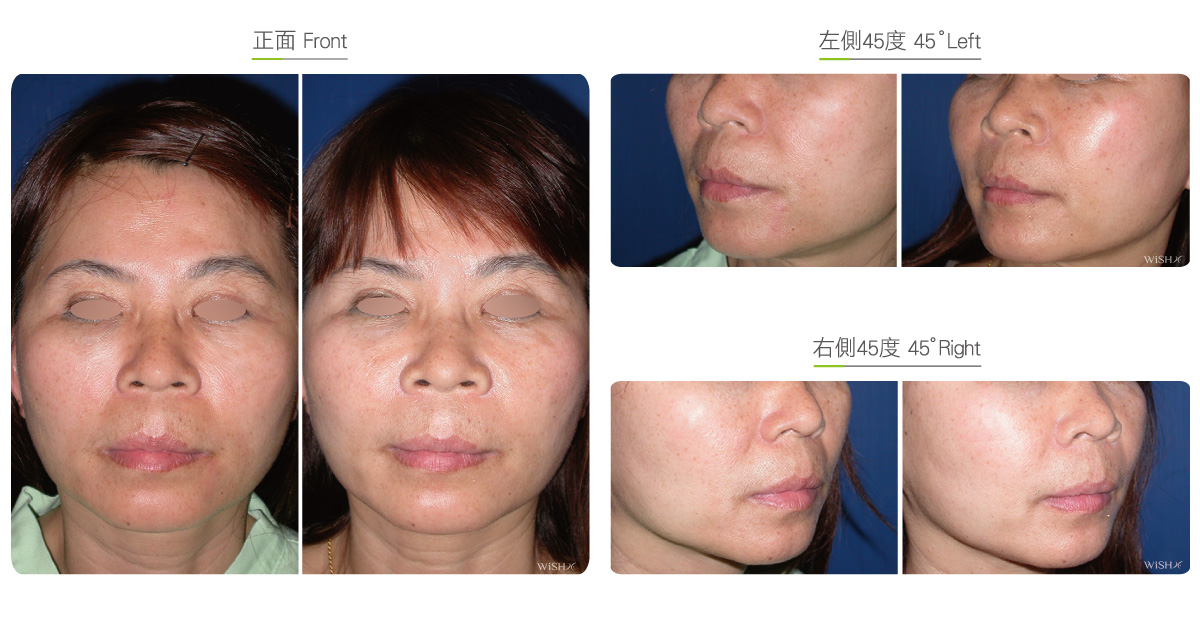
If the nasolabial folds of a patient are superficial static lines rather than an osseous depression, correction is conducted at the superficial skin structure, with the results more direct and effective than those obtained by paranasal augmentation. Traditionally, such a superficial layer surgery utilizes a simple injection of autologous fats to fill the nasolabial folds, but due to the frequent mouth motion, fats are prone to be absorbed or even completely drain away to present short results. Patients with long-term distinct nasolabial fold depression should consider undergoing wire scalpel (nasolabial fold knife) combined with autologous fat or fascia grafting, the results of which are superior to those obtained by simple fat injection and more stable and long lasting.
The so-called nasolabial fold knife is a particularly designed stainless steel saw, and at each end, it contains a long needle that can penetrate the dermal layer of the skin. The steel line connected to the long needle tail dissects and releases the skin to the bottom of the penetration area. It completely releases the tightly connected skin septa and ligaments below the nasolabial folds to fully separate the skin from deep tissues, so the nasolabial fold becomes shallow and fuzzy immediately. However, to avoid the recurrent adhesion of the nasolabial fold skin to below the muscles, the nasolabial fold knife should be frequently combined with autologous fat or strip fascia grafting to prevent the probability of skin adhesion and the occurrence or relapse of nasolabial folds. In general, this surgery improves superficial nasolabial folds by over 60%.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Type of incision: A 2-mm skin incision at both ends of the nasolabial folds Umbilicus (incision for fat grafting) or gluteal folds (incision for dermal fascia)
- Recovery: 5–7 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Try to avoid excess ice compresses and prohibit hot compresses after the operation.
- Avoid frequent motions of the mouth or food intake for 1 month postoperatively to prevent fat loss.
- Avoid smoking, alcohol, and irritating foods for 1 month postoperatively.
- Avoid heavy massage to or squeezing of the nasolabial folds for 3 months postoperatively.
Ideal candidates
- Patients with mild or superficial nasolabial folds
- Those with nasolabial folds and concurrent skin aging or laxity
- Those with aggravated nasolabial folds due to buccal droopiness
- Those unable to receive prosthesis implantation
- Those who have received an injection of hyaluronic acid or fats, the results of which are poor
Possible complications
- Skin adhesion
- Injection hole scar
- Fat self-absorption
- Excessive loss
- Lumps
- Recurrence of nasolabial folds
Surgical advantages
-
There are no risks of prosthesis implantation such as infection or dislocation.
-
It mitigates the excess absorption or loss that arises from a single autologous fat injection.
-
It effectively prevents or avoids the recurrence of nasolabial folds.
-
Surgical results are natural and free of foreign body sensation.
Surgical drawbacks
-
It is not suitable to resolve the osseous structural problems of a paranasal depression.
-
An incision scar may be left at both ends of the nasolabial folds.
-
Excess fat grafting may lead to lumps at the nasolabial folds or a facial expression change.
-
The absorption of fats or fascia may vary along with individual constitution.
-
It is not applicable to patients with very loose skin around the nasolabial folds.