Lip Functional Correction
The human lips are encircled by 12 muscles, and each muscle acts on the lip to cause numerous facial expressions. The malfunction of some muscles disrupts the containment and balance functions of each muscle group, which causes the lips to be skewed or deflected in a certain direction on speaking, resulting in disturbances of mouth skew or deviation. At present, the pathogenesis of such lip malfunctions remains unclear. Most cases are caused by viral infections during childhood or abnormal terminal motor neuron discharge, while some are caused by trauma. It is also frequently misdiagnosed as stroke in the early stage. However, different from facial palsy after stroke, such patients have a normal intake function and mostly facial expressions and appear without anomalies if they are not speaking and only show lip deflection toward a certain direction at the mouth opening, which is a result of excess discharge or spasm of facial expression muscle groups. Such signs are completely different from the difficulty in opening the mouth or even concurrent semi-facial muscle weakness due to cerebral nerve dysfunction among stroke patients. Therefore, differential diagnoses should be made correctly before lip functional correction.
The surgical correction should be adjusted in light of patients’ symptoms. For patients with unclear symptoms, Botox injection is a good tool for the differential diagnosis of muscular groups. If the problem is identified due to certain muscles, surgery is conducted. Muscle groups with an inertial spasm or a contracture are regionally severed and resected. Most frequently, the surgery is targeted at the spasticity of the levator anguli oris or depressor anguli oris, where Dr. Chuang localizes the muscle with an electric nerve stimulator, creates a 1-cm incision inside the lip at the localized area, and then separates the abnormal muscle under a microscope to sever it. This procedure avoids injuries to other muscle groups with normal functions. Meanwhile, patients should stay lucid during the operation and make various lip motions in line with the instructions provided by Dr. Chuang to help confirm the location and running direction of the problematic muscle. Generally, once excised, excessively contracted muscle groups immediately return to normal, so patients can attain significant improvement soon after the operation.
Surgical conditions
Duration
- Type of anesthesia: Local anesthesia
- Type of incision: Approximately 1-cm incision at the inner margin of the lip
- Recovery: 1–2 days
- Removal of stitches: No
General instructions
No food and water on the day of surgery
- Avoid smoking, alcohol, and irritating foods for 1 month postoperatively, and avoid singing or laughing and other overt mouth opening behaviors.
- Frequently perform mouth rehabilitation exercises for 6 months postoperatively to strengthen the functions of the balancing muscles.
Ideal candidates
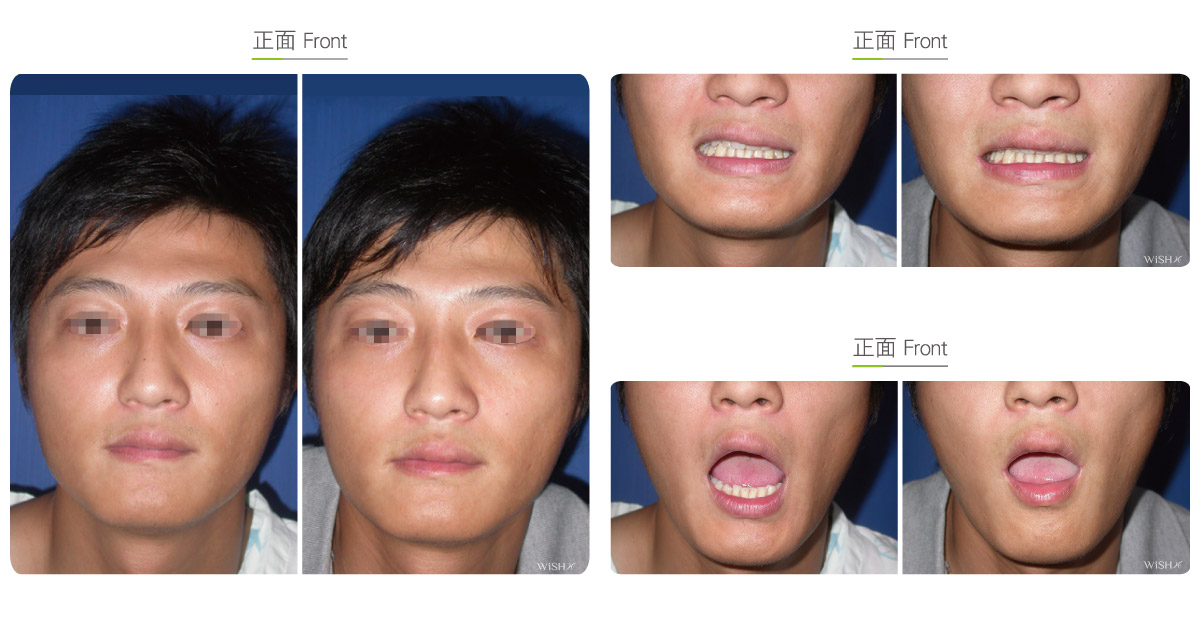
- Patients whose mouth corner shows a deviation or deflection toward a certain direction on opening the mouth
- Those unable to consciously control the degree of mouth corner deviation.
- Those whose lips appear deviated due to a consistent muscular stretch even without making any facial expression
- Those with an obvious mouth deviation that may undermine the self-confidence or normal social interaction
Possible complications
- Lip muscle contracture
- Excess or incomplete correction
- Recurrence due to muscular adhesion
Surgical advantages
-
It resolves the long-term disturbance of mouth deviation.
-
Surgical results are immediately noted.
-
It is the least invasive method and requires almost no time for recovery.
Surgical drawbacks
-
It is difficult to localize the lip muscles, which may lead to incomplete correction.
-
The excess resection of lip muscles may occur to cause compensatory stretching of the contralateral lip.
-
A probability of recurrence still exists (approximately 10%)