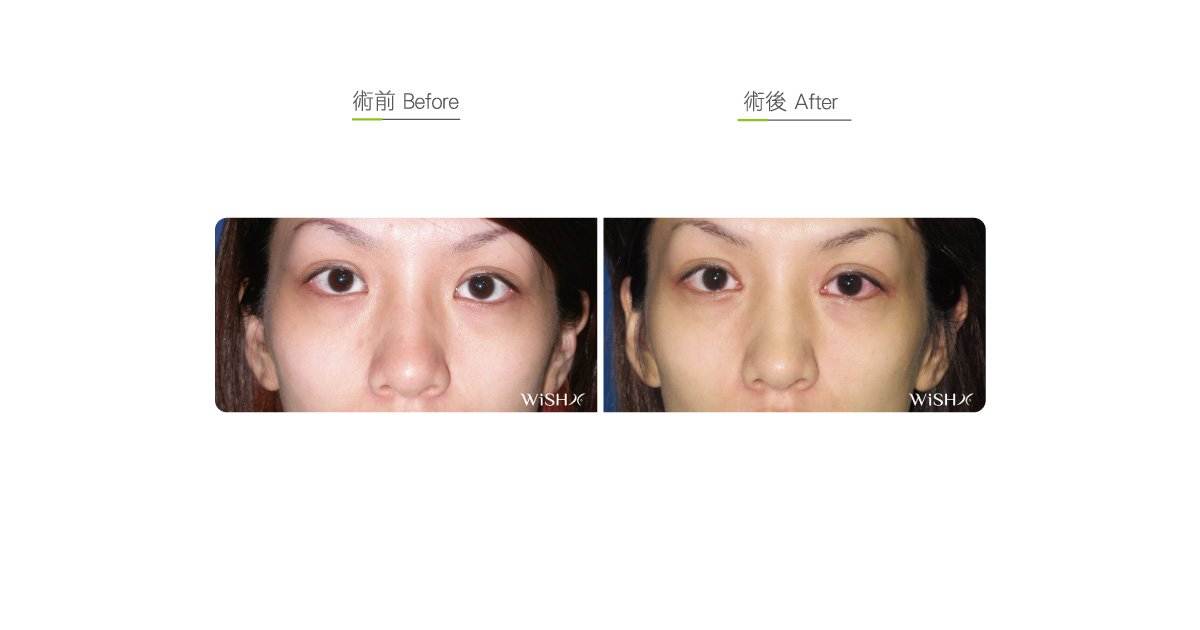
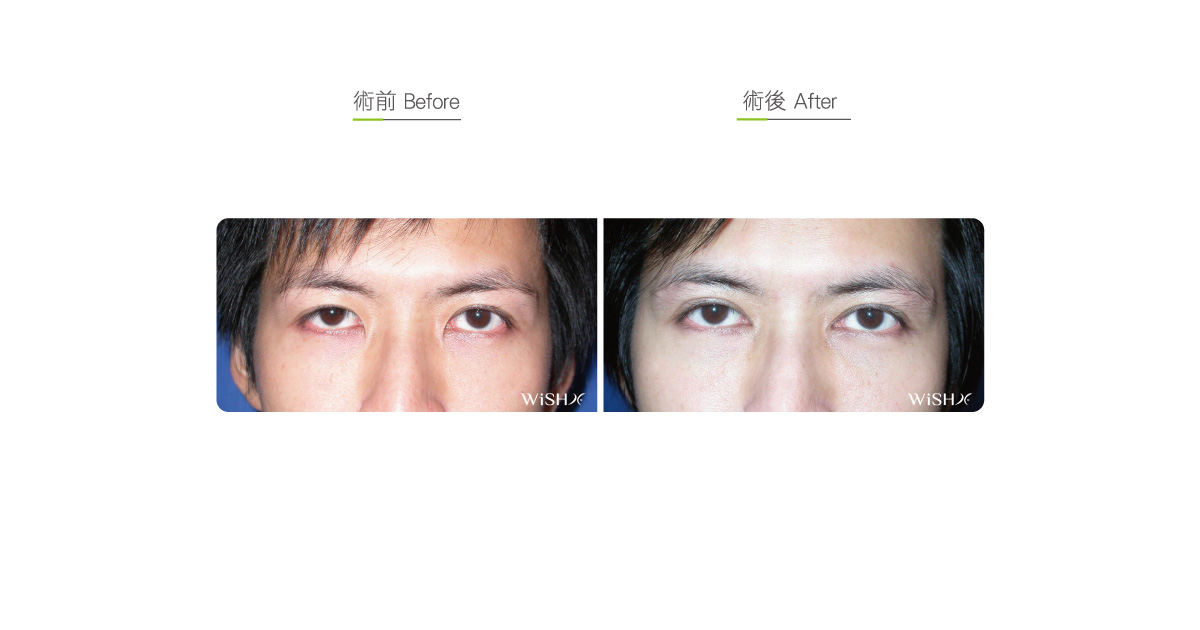
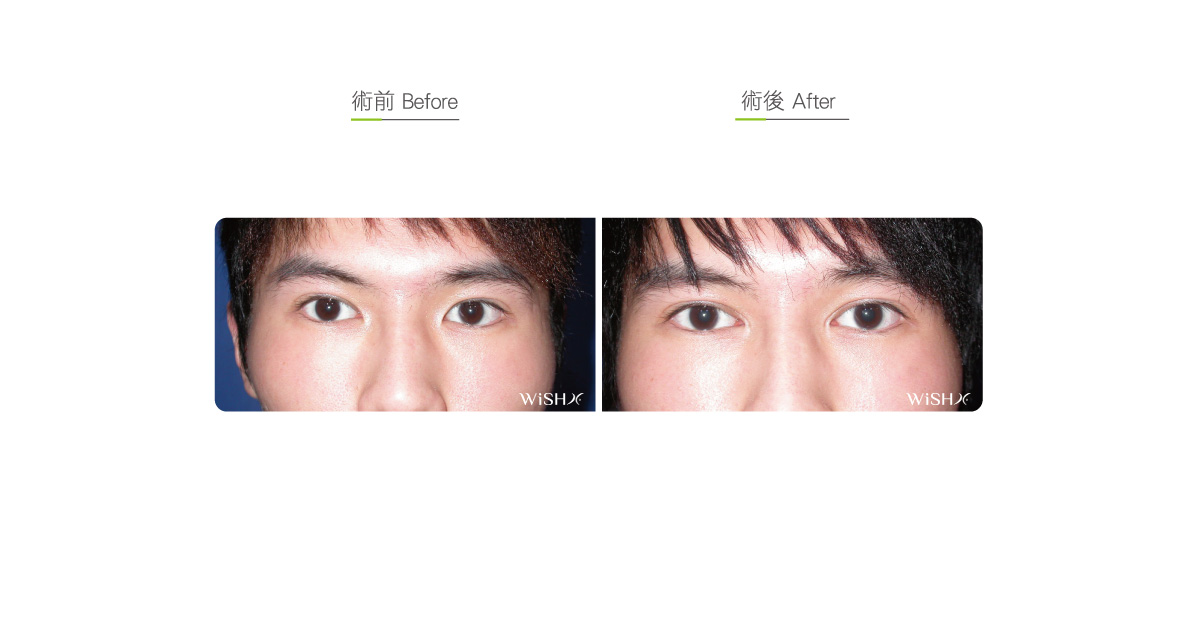
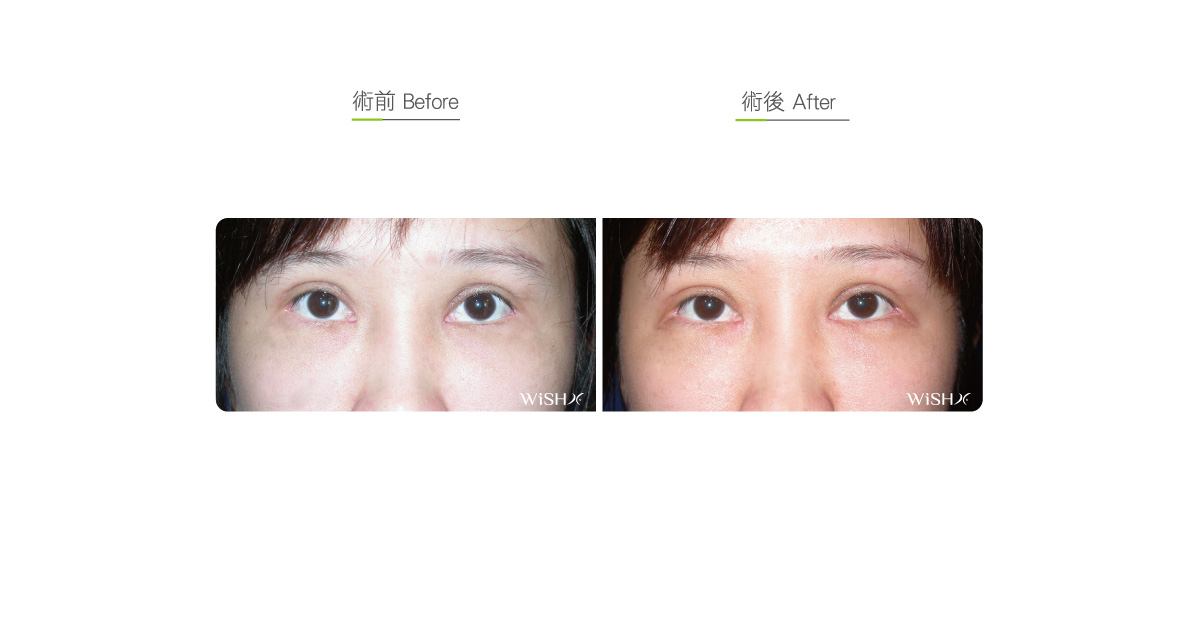
Medial Canthoplasty (Epicanthoplasty)
The inner eye corner, also called the medial canthus (corner), is mostly covered by a patch of thick skin among Orientals, which is commonly called the Mongolian fold. This has also given rise to the name almond or Phoenix eye. If it is too thick or tight, the skin can limit the eye size or cause an exceedingly wide interocular span; in severe cases, it can also affect the smoothness or naturalness of acquired double eyelid folds. Therefore, on consultation with patients about double eyelid surgery, the physician should also evaluate the necessity of medial canthoplasty. According to Dr. Chuang’s experience, appropriate medial canthoplasty adds the final touch to enhance the elongation effects of double eyelid folds and enlarges the eyes to make the original lusterless eyes bigger and brighter. Therefore, many patients choose to undergo concurrent medial canthoplasty and double eyelid surgery to maximize the postoperative results.
Besides enlarging the eyes, medial canthoplasty changes the eye shape or double eyelid patterns. Generally, for patients having almond eyes with a thick medial canthus, folds at one-fifth of the inner canthus are naturally embedded in the epicanthal skin after double eyelid surgery, which is the so-called close pattern double eyelids (or Asian’s double eyelids) and is the common double eyelid appearance among Orientals. Despite natural results, it is unable to change the interocular span or eye size. If the medial canthus is dissected, the double eyelid fold extends to the deep inner eye corner and is not covered by the Mongolian fold at the inner eye corner, which then results in sculpting open-pattern double eyelids like Caucasians or mixed blood individuals (called parallel double eyelids) or even simultaneously adjusts the running direction or level of the medial canthus to customize the eyes to be suitable to oneself. Thus, this method is popular among females who would like to have big and bright eyes.
There are numerous surgical methods for medial canthoplasty. At present, Dr. Chuang mainly utilizes w-plasty medial canthoplasty. This technique requires first excising the partial excess skin at the medial canthus and then tightening and stitching the transversely dissected inner canthus to the superior and inferior skin defects and aligning with the double eyelid folds. This is a relatively subtle minimally invasive medial canthoplasty. Its advantage is that the angle and extent of medial canthus dissection can be flexibly adjusted, which does not cause excess inward correction or caruncle exposure, frequently reported in the traditional medial canthus cutting procedure. Besides, the incision can be completely aligned with the double eyelid folds to prevent complications such as unsmooth medial canthal folds or scar exposure. Additionally, the surgical results are natural, which avoid cat’s eye, fox’s eye, or cross-eye. It is highly safe and also able to meet the requirements of an overwhelming majority of patients concerning eye shape. Regarding drawbacks, it requires complex stitching and accurate alignment of the skin fold, so the surgical procedures are complicated. Moreover, a short stitched wound is exposed at the skin inferior to the medial canthus, which leaves a temporary scar and needs 3–6 months to gradually fade before becoming invisible to the naked eye.
Moreover, for some patients with an overtly round inner canthus or a poor angle that does not require a substantial modification of the medial canthus, Dr. Chuang utilizes z-plasty medial canthoplasty for the fine adjustment of the medial canthus. This method is mainly aimed to change the running direction and pointedness of the inner corner and does not require much skin resection, so the scar is less visible than that from w-plasty but presents risks such as overcorrection or exceeding concentration of the medial canthus. It is suitable for patients having unobvious Mongolian folds, a concentrated interocular span, a scarring tendency, or a small medial canthus revision. Its drawbacks are that the results are relatively conservative and limited and that the tip of the medial canthus points slightly downward. Therefore, the physician must control the degree of dissection to not cause unnatural results.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Surgical incision: At the skin of the medial canthus
- Recovery: 2–-3 days
- Removal of stitches: 7 days
General instructions
No food and water on the day of surgery
- Avoid smoking, alcohol, and irritating foods for 1 month postoperatively.
- Continue scar care for 3 months postoperatively to avoid scarring.
Ideal candidates
- Patients with exceedingly small and round eyes
- Those with an exceedingly wide interocular span that makes both eyes look lusterless or apathetic
- Those who like open or parallel double eyelids
- Those with a congenital downward medial canthus that makes the eyes look like cat’s eye or fox’s eye
- Those who underwent have undergone double eyelid surgery but presented unsmooth or multilayered medial canthal folds
- Those with mild esotropia or cross-eye
- Those who would like extreme enlargement of the eyes
Potential complications
- Scar hypertrophy
- Excess correction
- Exceedingly narrow interocular span
- Exceedingly pointed medial canthus
- Exposure of caruncle
Surgical advantages
-
It distinctly enlarges the eyes and shortens the interocular span to make the eyes appear concentrated.
-
It is performed along with double eyelid surgery to sculpt open- pattern double eyelids (parallel double eyelids).
-
It adjusts the running direction and angle of the medial canthus and remedies the congenital apathetic or sharp eye shape.
-
It avoids bifurcation or unevenness of medial canthal folds resulting in of the ddouble eyelid surgery.
-
It partially adjusts the appearance of esotropia (cross-eye).
-
It partially corrects eyelash inversion
Surgical drawbacks
-
The Ttemporary scar needs approximately 3–6 months to subside and disappear.
-
Excess medial canthoplasty may lead to the exposure of the caruncle or increased secretions at the medial canthus due to chronic as well as other complications like such as corneal irritation.
-
The Ssurgical results are irreversible and difficult to restore in the future.
-
Permanent scars may be left.