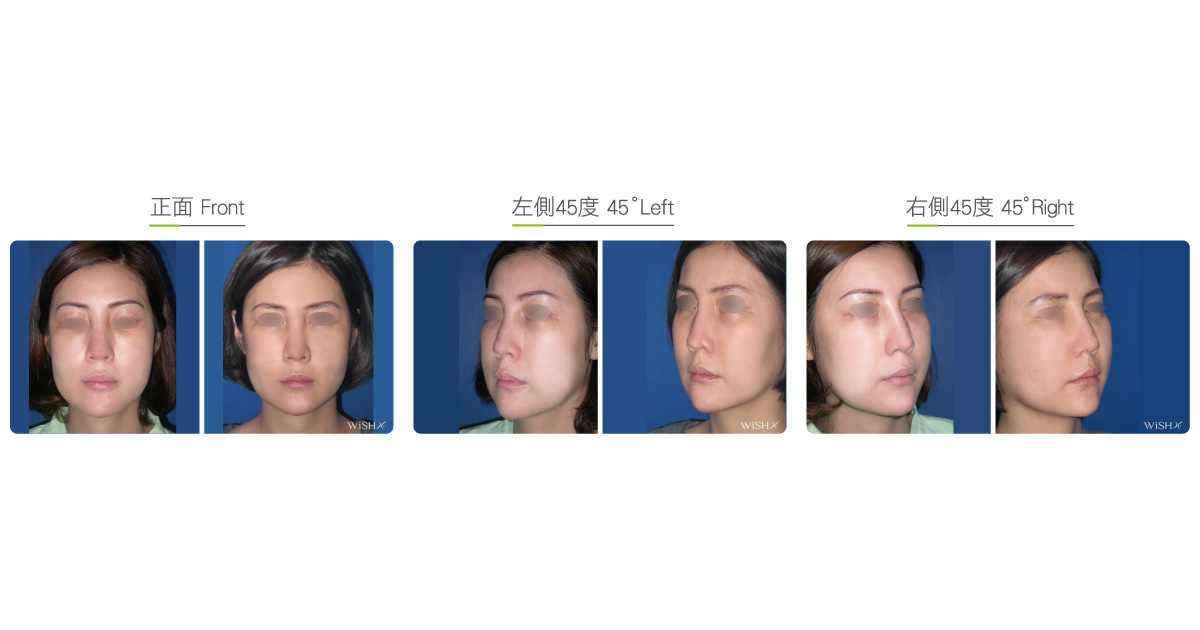
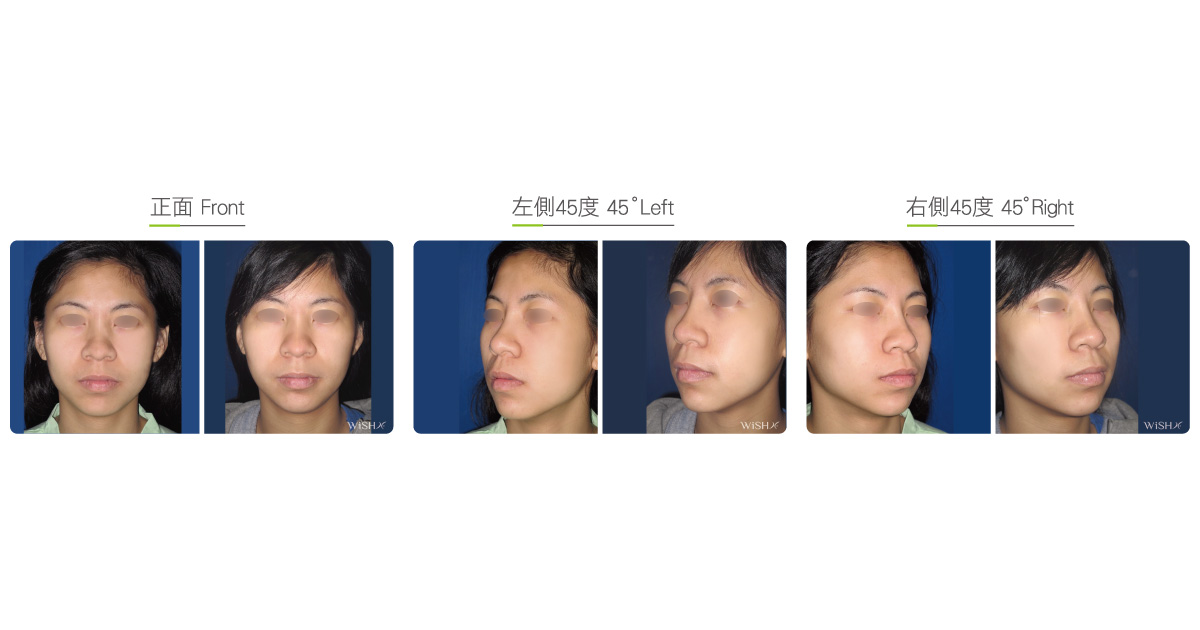
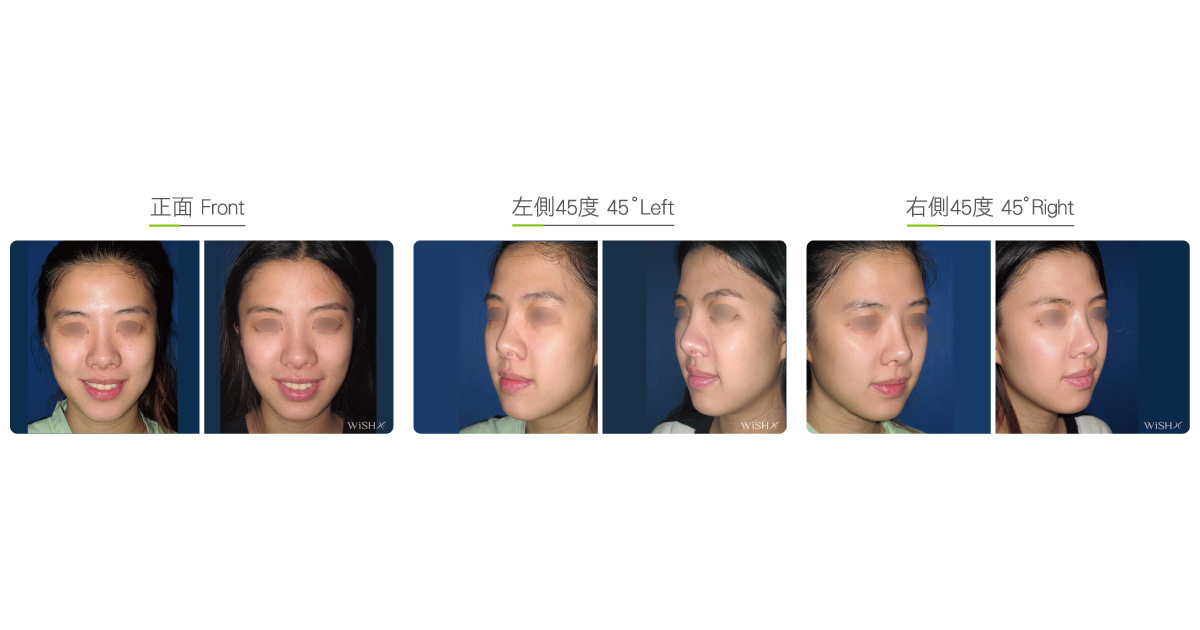
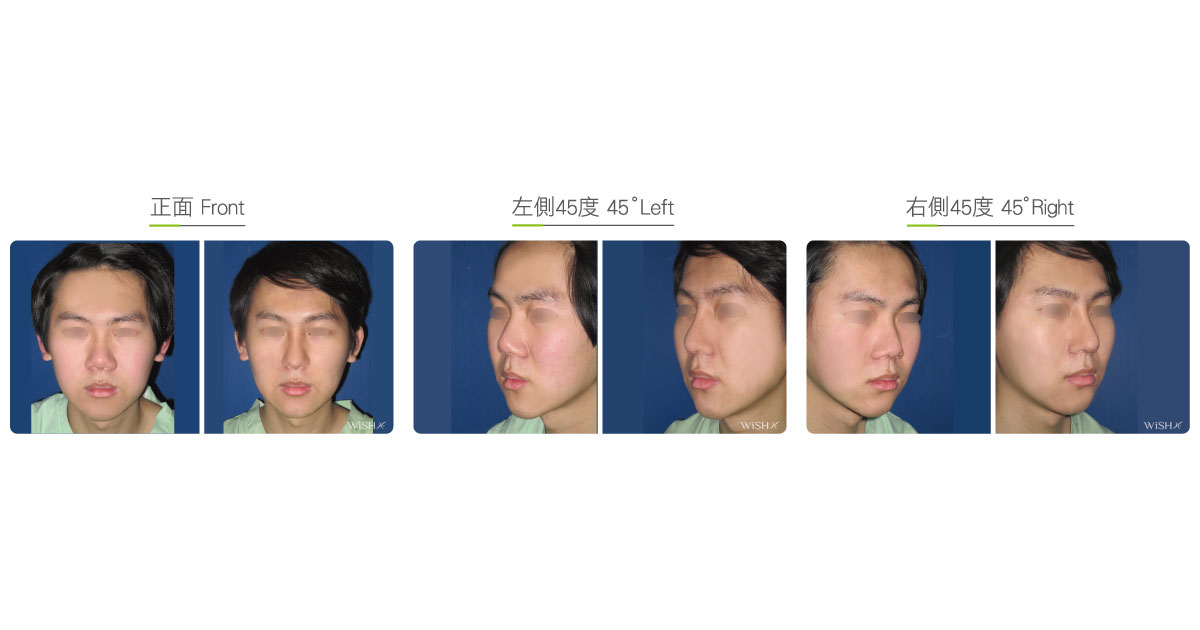
Buccal fat pad removal
Buccal (intraoral) fat pads are at deep tissues inside the oral cavity rather than at the superficial fat layer under the skin. They are less prone to change along with body weight and exist after the development of puberty. Anatomically, they are distributed between the masticatory muscle and mandible bone, namely the middle one-third portion of the lower face, and primarily serve to cushion the cheek and gingiva as well as protect the teeth from collision. Buccal fat pads protrude outward from the face due to obesity, excess mastication, aging, or fat pad looseness because of facial bone reduction and commonly manifest as buccal hypertrophy (commonly called chubby face or baby fat) or two protruding lumps at both sides of the mouth corner on smiling (also called circumoral fat), thus making the lower cheek appear sagged and bulging. Therefore, patients should consider undergoing buccal fat pad removal to alleviate weight loads inside the cheek and prevent the future probability of continuous buccal sagging.
This surgery involves creating a 1-cm incision at the buccal mucosa inside the oral cavity; via this incision, deep buccal tissues are separated with the assistance of a headlamp illumination, and buccal fats are identified near the masticatory muscle and removed in chunks. For patients with a relatively thin skin or mild circumoral fats, they consider preserving one-third portion of the fat pads to avoid future skin laxity or buccal depression.
Limited in distribution area, buccal fat pads differ from facial subcutaneous fat accumulation in skin hypertrophy as well as the treatment method, so the physician needs to conscientiously conclude the diagnosis before surgery. Based on Dr. Chuang’s experience, patients with a round face or an obese stature are prone to have concurrent extensive subcutaneous fat accumulation, so facial liposuction should be considered first; if the patient’s skin is normal but appears as regional fats protruding outward from both cheeks that become more obvious on making facial expressions or smiling, it is highly likely to be caused by buccal fat pad protrusion, so an intraoral incision should be made to remove the fat pad. In clinics, there are a minority of patients undergoing combined subcutaneous fat hypertrophy and intraoral fat pad protrusion, and the physician should notify the patient of the severity and treatment results before deciding to resolve such facial hypertrophies in sequence or at one time.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia
- Type of incision: A 1-cm incision at the intraoral mucosa
- Recovery: Within 2–3 days
- Removal of stitches: No
General instructions
No food and water on the day of surgery
- Try to avoid hard food or food that is hard to chew for 1 week postoperatively.
- Try to avoid smoking, alcohol, or other irritating foods for 1 month postoperatively.
Ideal candidates
- Patients with obvious baby fat or circumoral fats at both cheeks
- Those with protruded curves at both cheeks on smiling or making facial expressions
- Those with a round or pancake face and combined buccal hypertrophy
- Those who have undergone facial liposuction that resulted in insignificant face slimming
- Those willing to undergo facial bone reduction and wishing to prevent skin sagging
- Those aspiring to have an extremely slim or sharp face
Possible complications
- Buccal depression
- Skin laxity
- Results short of expectation
Surgical advantages
-
It effectively solves the long-term disturbance of baby or circumoral fats.
-
It alleviates buccal load and prevents future skin aging and sagging on the lateral cheeks.
-
It enhances the face slimming effect of Botox or the results of bone reduction.
-
It prevents skin laxity or droopiness after facial bone reduction.
-
Its facial slimming effect is more obvious than that from facial liposuction.
Surgical drawbacks
-
Excessive fat removal may lead to buccal depression.
-
Face slimming effects may be subtle in patients with a big or broad face.
-
It is not indicated for patients with an obvious round face or obesity.
Possible procedures in conjunction
Comparison of facial hypertrophy treatments
| Facial liposuction | Buccal fat removal | Lipodissolve injection | |
|---|---|---|---|
| Ideal candidates | Patients with a round face, pancake face, and thick facial skin (>1 cm) | Patients with regional buccal hypertrophy or protrusion and baby or circumoral fats | Patients with heavy cheeks or mild hypertrophy or regional fat accumulation |
| Characteristic symptoms | Change along with the face but not with facial expressions | Exist regardless of fat or thin skin and protrudes more obviously on smiling | Change along with the face but not with facial expressions |
| Treatment method | Liposuction | Incisional fat pad removal | Subcutaneous injection |
| Treatment target | Superficial fat | Intraoral deep fat | Superficial fat |
| Surgical principle | Negative pressure suction of fat globules | Removal of fat chunks | Lipolysis and metabolism |
| Surgical scope | Whole cheek or chin | Middle segment of the lateral cheek | Whole cheek or chin |
| Surgical incision | Approximately 2-mm needle hole at the inferior margin of the earlobe or chin | Approximately 1-cm incision at the intraoral mucosa | No |
| Anesthesia method | IV sedation + local anesthesia | IV sedation + local anesthesia | Topical anesthesia |
| Postoperative recovery | 3–5 days | 2–3 days | 2–3 days |
| Postoperative stitch removal | Yes | No | No |
| Repeat treatment | No | No | Once every month |
| Buccal depression | No | Probable | No |
| Recurrent hypertrophy probability | Low | No | Relatively high |
| Concurrent surgery | Mid and lower face lift and jawline lift | Cheek bone and mandible reduction | No |