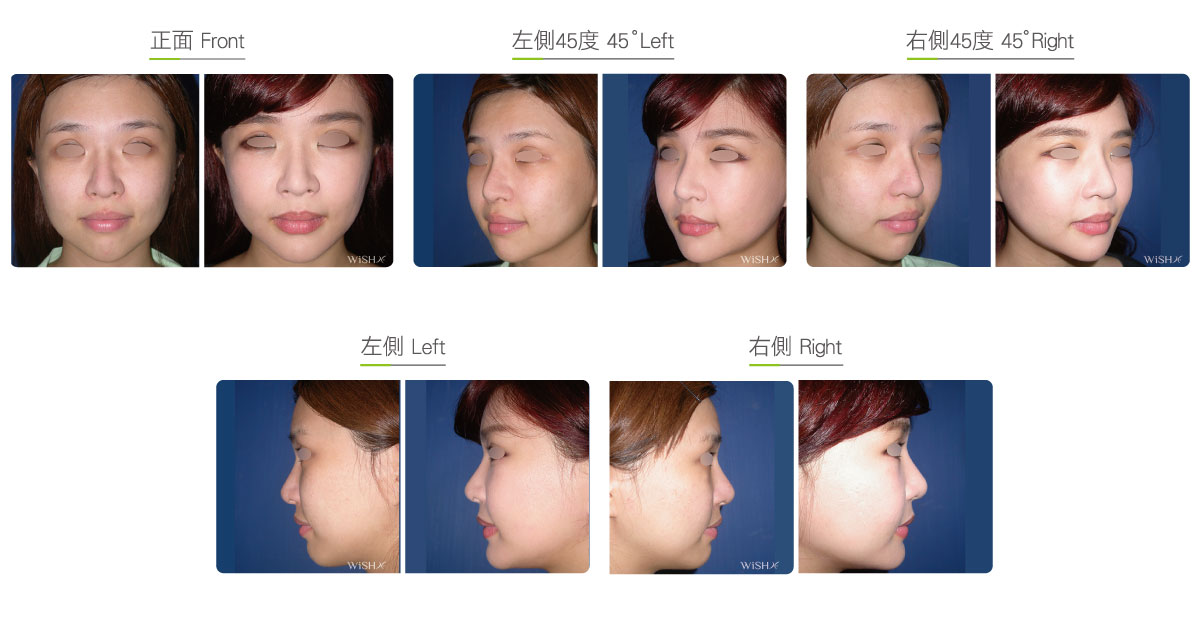
Forehead/Temporal/Malar/Cheek Augmentation
The face is where autologous fats are commonly injected. It includes the forehead, temple (marriage palace), both cheeks, nasolabial folds, submalar triangle, and even the nose, chin and eyelids, which could be filled, reinforced, or enhanced by the injection of proper amounts of fats. In particular, due to the predisposition to cheek and temple depression because of facial bone features, orientals are most suitable for fat grafting because congenitally very broad cheek bones result in bilateral buccal sinking, drastic weight loss that leads to buccal fat atrophy, or aging that gives rise to a gradual loss of facial collagen and fats. Such patients are mainly aged 30–60 years, and the priority correction method is the restoration of soft tissue volume. Despite nonsurgical injections such as hyaluronic acid, collagen, 3D sculptra, and other synthetic injectables, they only provide temporary improvement, and repeatedly long-term injections are expensive. Therefore, patients with extensive and severe buccal depression should first consider filling by an autologous fat injection, which not only provides more comprehensive and longer results than injectables but also is more economic.
Regarding cheek fat augmentation, proper fats should be collected from the abdomen or thigh of patients, and after filtrating, prime adipocytes are selected and mixed with growth factors derived from the patient’s plasma in a certain proportion, which is then directly injected into the cheek depression via a fine injection needle. Despite no limitation on the area of fat grafting, such as at the forehead, temple (marriage palace), lateral cheeks, nasolabial folds, and submalar triangle, injections to some sites such as the anterior area of lower cheeks, nasolabial folds, and submalar triangle should be moderate; otherwise, it is likelier to cause premature skin droopiness and other complications. Additionally, the adipocyte survival rate varies at different body parts. For areas where results are relatively stable such as the forehead, temple, and submalar triangle, the self-absorption rate is controlled and is below 40%, while the adipocyte survival rate at the bilateral cheeks is relatively low, at approximately 50%, and the nasolabial folds or posterior area of the cheek is most susceptible to fat loss due to the frequent motion of the mouth, with the adipocyte survival rate at 30–40% on average.
Despite advantages in the convenient source of fats, the self-absorption degree cannot be fully controlled after the injection of adipocytes, so Dr. Chuang injects relatively more fats into affected sites to prevent excess fat absorption. Generally, the amount of fats necessary for forehead or temple augmentation is approximately 30 cc, that for both cheeks is approximately 10–15 cc, and that for nasolabial folds in only 5–8 cc; therefore, at most, 50 cc of purified fats is required for fat augmentation of the whole face. Moreover, adipocytes transferred to the cheeks mostly begin to regrow within 1 month and achieve 80–90% stable conditions within 3 months. The final result becomes fixated within 6 months at most and not absorbed. Therefore, if the fat survival rate can be maintained at over 50% for 6 months postoperatively, results are generally sustained for 3–5 years. Dr. Chuang recommends that patients should maximally avoid drastic body weight decrease or staying up late and alcohol abuse after the operation; otherwise, fats are prematurely absorbed, thus undermining surgical results.
Surgical conditions
Duration
- Type of anesthesia: IV sedation + local anesthesia or general anesthesia
- Type of incision: A 2-mm needle hole on the face or hairline
Wound for the collection of fats (approximately 5 mm)
- Recovery: 5–7 days
- Removal of stitches: 5–7 days
General instructions
No food and water on the day of surgery
- Avoid excess cold or hot stimulus to the fat filling sites on the day of operation.
- Avoid heavy compression to the face or massage for 1 month postoperatively.
- Avoid drastic facial expressions or chewing for 3 months postoperatively.
Ideal candidates
- Patients with sunken cheeks or temples due to congenitally prominent facial bones
- Those with rapid facial fat loss due to weight decrease or loss
- Those with facial fat and collagen loss due to skin aging or laxity
- Those willing to correct a congenital midface depression or an excessively long face appearance
- Those willing to correct a congenitally projected maxilla or excessively deep nasolabial folds
- Those who want to augment or plump up the forehead and temples
Possible complications
- Fat absorption
- Fat obesity
- Uneven absorption
- Subcutaneous lumps
- Premature skin droopiness
Surgical advantages
-
One surgery realizes the filling of multiple sites, and results are extensive and the process economic.
-
Surgical results last for a longer time than those obtained by filler injections.
-
Because of complete autologous cell transplantation, there is no risk of rejection or infection.
-
Results are more natural than those obtained with foreign prostheses.
-
It is combined with the liposuction of obese body parts.
Surgical drawbacks
-
Self-absorption of fats may occur, and the degree may vary along with individual condition.
-
Excessive injection may cause subcutaneous lumps or obesity temporarily.
-
Fat mass may increase the skin load, thus resulting in premature droopiness of cheek.
-
Fat absorption may be uneven, and revision surgery and adjustment may be necessary.
-
Fats may change along with body weight, so long-term results are difficult to evaluate.